


Hepatitis B Vaccine for Infants
Is it worth it?

When parents begin their research into vaccines, I often recommend starting with the Hepatitis B vaccine because this is the one they will be pressured to consent to before their newborn infant is released from the hospital. Researching the Hepatitis B vaccine is also important because it gives a good bit of information on how the CDC (Centers for Disease Control) and the ACIP (Advisory Committee on Immunization Practices) conduct themselves when it comes to vaccines in general.
In 1991, the American Council on Immunization Practices (ACIP) recommended universal vaccination of all U.S. infants with 3 doses of hepatitis B vaccine, beginning within 48 hours of birth. Hepatitis B is a sexually-transmitted disease and is spread the same way HIV and Hepatitis C are spread: through contact with body fluids such a semen, vaginal fluids, and blood. Those at high risk of infection include homosexual men, heterosexuals who have multiple sex partners, and healthcare workers who are exposed to body fluids. Infants whose mothers are actively infected with Hepatitis B are at increased risk of infection. This is what the CDC has to say about Hepatitis B infection.
Pregnant women in the U.S. are screened for Hepatitis B infection.
Infants who are born to mothers who are not infected with hepatitis B are at very low risk for infection, by virtue of the fact that they are not engaging in high-risk behaviors that are associated with hepatitis B. (i.e., Infants are not having sex and they are not using injection drugs.)
The CDC states that the incidence of hepatitis B infection in U.S. children (age 0-19 years) decreased by 89% between 1990 and 2002 as a result of mass vaccination of infants. This is misleading, in my opinion. When you say that the incidence of the illness decreased by 89% it sounds like the vaccine has been extremely effective in improving the health of children who receive it. The opposite is actually the case.
Here are some studies that have investigated the health effects of hepatitis B vaccine in U.S. children:
· Controlling for age, race and gender simultaneously in the 1994 NHIS, hepatitis B vaccine was found to be associated with prevalent arthritis [odds ratio (OR) = 5.91], incident acute ear infections (OR = 1.60), and incident pharyngitis/nasopharyngitis (OR = 1.41). (citation)
· Hepatitis B vaccinated children had an unadjusted odds ratio of 2.94 and age-adjusted odds ratio of 2.35 for liver problems compared with non-hepatitis B vaccinated children in the 1993 National Health Interview Survey. Hepatitis B vaccinated children had an unadjusted odds ratio of 2.57 and age-adjusted odds ratio of 1.53 for liver problems compared with non-hepatitis B vaccinated children in the 1994 National Health Interview Survey Dataset. (citation)
· In people not previously exposed to hepatitis B, vaccination has unclear effect on the risk of developing infection, as compared to no vaccination. The risk of lacking protective antibody levels as well as serious and non-serious adverse events appear comparable among recipients and non-recipients of hepatitis B vaccine. (citation) (no benefit from receiving the vaccine)
· Engerix B vaccine appears to increase [risk of CNS inflammatory demyelination], particularly for confirmed multiple sclerosis, in the longer term. (citation)
· This study investigated the association between vaccination with the Hepatitis B triple series vaccine prior to 2000 and developmental disability in children aged 1-9 years (n=1824), proxied by parental report that their child receives early intervention or special education services (EIS)… The odds of receiving EIS were approximately nine times as great for vaccinated boys as for unvaccinated boys…This study found statistically significant evidence to suggest that boys in the United States who were vaccinated with the triple series Hepatitis B vaccine, during the time period in which vaccines were manufactured with thimerosal, were more susceptible to developmental disability than were unvaccinated boys. (citation)
· Boys vaccinated as neonates had threefold greater odds for autism diagnosis compared to boys never vaccinated or vaccinated after the first month of life. Findings suggest that U.S. male neonates vaccinated with the hepatitis B vaccine prior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period. (citation)
The last two articles listed above involved data analysis for children who received the hepatitis B vaccine prior to the elimination of Thimerosal, or mercury from the vaccine. This may lead you to believe once that was accomplished the problem was solved. The current hepatitis B vaccines contain high amounts of aluminum. The following articles have to do with the problems associated with aluminum in infant vaccines:
· In the present review we describe how the use of a systems biology approach in cultured hepatoblastoma cells (HepG2) allowed the identification of the molecular targets of Al toxicity. Mitochondrial metabolism is the main site of the toxicological action of Al. Fe-dependent and redox sensitive enzymes in the tricarboxylic acid (TCA) cycle and oxidative phosphorylation (OXPHOS) are dramatically decreased by Al exposure. In an effort to compensate for diminished mitochondrial function, Al-treated cells stabilize hypoxia inducible factor -1a (HIF-1a) to increase ATP production by glycolysis. Additionally, Al toxicity leads to an increase in intracellular lipid accumulation due to enhanced lipogenesis and a decrease in the B-oxidation of fatty acids. Central to these effects is the alteration of a-ketoglutarate (KG) homeostasis. In Al-exposed cells, KG is preferentially used to quench ROS leading to succinate accumulation and HIF-1a stabilization. Moreover, the channeling of KG to combat oxidative stress leads to a reduction of L-carnitine biosynthesis and a concomitant decrease in fatty acid oxidation. The fluidity and interaction of these metabolic modules and the implications of these findings in liver-related disorders are discussed herein. (citation) (Marcella’s Note: The importance of these findings is relevant especially for brain development and for chronic autoimmune disorders such as diabetes and autism. The disruption of mitochondrial metabolism is significant in the increased risk of vaccine-injury in persons who have underlying mitochondrial disorders – See the Hannah Poling case for more information.)
· When assessing adjuvant toxicity in children, several key points ought to be considered: (i) infants and children should not be viewed as “small adults” with regard to toxicological risk as their unique physiology makes them much more vulnerable to toxic insults; (ii) in adult humans Al vaccine adjuvants have been linked to a variety of serious autoimmune and inflammatory conditions (i.e., “ASIA”), yet children are regularly exposed to much higher amounts of Al from vaccines than adults; (iii) it is often assumed that peripheral immune responses do not affect brain function. However, it is now clearly established that there is a bidirectional neuro-immune cross-talk that plays crucial roles in immunoregulation as well as brain function. In turn, perturbations of the neuro-immune axis have been demonstrated in many autoimmune diseases encompassed in “ASIA” and are thought to be driven by a hyperactive immune response; and (iv) the same components of the neuro-immune axis that play key roles in brain development and immune function are heavily targeted by Al adjuvants. In summary, research evidence shows that increasing concerns about current vaccination practices may indeed be warranted. Because children may be most at risk of vaccine-induced complications, a rigorous evaluation of the vaccine-related adverse health impacts in the pediatric population is urgently needed. (citation)
With all of these concerns about the safety of aluminum in vaccines, and about the Hepatitis B vaccine in particular, you may be led to ask yourself, “Is it worth it?”
As noted above, the CDC states that the incidence of hepatitis B infection in U.S. children has decreased by 89% as a result of mass vaccination. What does this really mean?
In 1990, the incidence of hepatitis B infection in U.S. children between birth and 19 years of age was 3.03 per 100,000. In 2002, the number had declined to .34 per 100,000 (citation). This is how they came up with the 89% decrease. Another way of putting this is that if the 1990 number had been 1 infection out of 1 million people, and mass vaccination had wiped out that 1 instance of infection over a period of 12 years, the CDC would be claiming the vaccine was responsible for a 100% decrease in hepatitis B infection.
Can we really credit the vaccine with the reduction in cases? Look at the following two graphs from the CDC. The first is the graph of Hepatitis B and the second is the graph of Hepatitis C.
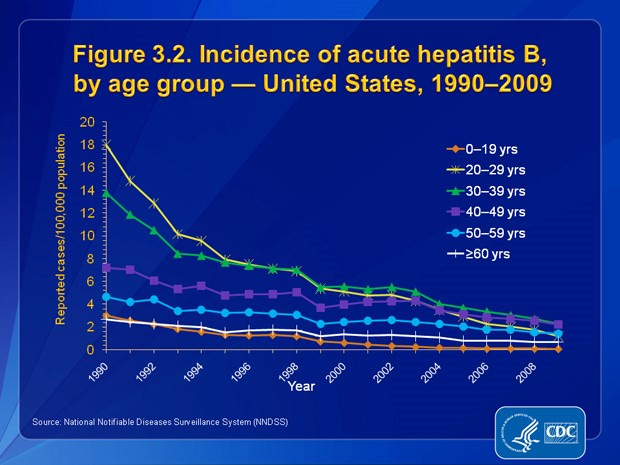
Source: https://www.cdc.gov/hepatitis/Statistics/2009Surveillance/Slide3.2.htm
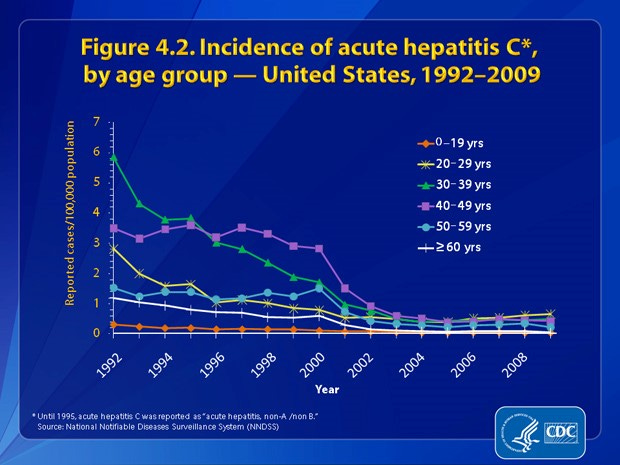
Source: https://www.cdc.gov/hepatitis/Statistics/2009Surveillance/Slide4.2.htm
Hepatitis C has decreased at a comparable rate to Hepatitis B, but there is no vaccine for hepatitis C. This suggests that the decrease in incidence is not due to the vaccine, but due to other factors, such as increased awareness of the dangers of unprotected sex among those groups who are at highest risk of contracting both hepatitis B and hepatitis C.
The CDC reported a total of 10,637 cases of acute hepatitis B disease in 1996, with 279 of those cases in children under 14 years of age (citation). Using these numbers, we can calculate the percentage of cases of hepatitis B disease that occur in U.S. children between birth and age 14 as 2.62%.
To get an idea of the true decrease as a result of vaccination, we need to look at the data beginning before the mass vaccination of infants. In 1990, the overall rate of hepatitis B infections reported in the U.S. was 21,102 (citation). Using the 2.62% rate, we can estimate the number of cases in children under 14 as 552.87 or 553 cases.
In 2002, the overall rate of hepatitis B infections reported in the U.S. was 8,064 (citation). Using the 2.62% rate, we can estimate the number of cases in children under 14 as 211.27 or 211 cases.
So, from 1990 through 2002, we can estimate that the number of cases of hepatitis B infection per year in U.S. children between birth and 14 years of age decreased by approximately 230 cases.
In general, children who are infected with hepatitis B tend to experience a milder course of disease than adults do. We know that among adults with hepatitis B infection, approximately 5% do not recover completely. The other 95% have no lasting problems. Among the 5% who do not have a complete recovery, 5% become chronic carriers, and 25% of them will die from liver cancer that develops decades later in life (citation). (Note: Since the first writing of this article, the CDC has changed its numbers and now estimates that 2-6% of adults with hep B become chronic carriers. For the purpose of these calculations, I will be sticking with the 5% they originally reported, understanding that there is a variance, which may mean the numbers are considerably lower or slightly higher.) Using the numbers from 1990 (the year before the vaccine was recommended for universal use in infants) we can estimate the overall rate of death from hepatitis B as follows:
1990 infections = 21,102
5% do not recover completely = 1,055
5% of them become chronic carriers: 1,055 x .05 = 53
deaths from liver disease later in life: 53 x .25 = 13
But what about Hepatitis B cases in children, since our infants are the ones who are accepting the major risk from vaccination against hepatitis B disease?
What is the risk to infants in the U.S., when it comes to dying from hepatitis B infection?
If we compare the numbers from 1991 to 2011 (a 20-year span) and we estimate that approximately 230 cases of hepatitis B per year have been prevented in children as a result of mass vaccination, we can estimate that the total number of cases of hepatitis B that have been prevented in children is 4,600 cases (230 x 20).
We know that children generally have a milder case of the disease than adults, but we don’t have a number for that, so we’ll go with the higher number of 5% becoming chronic carriers.
4600 x .05 = 230 (5% who do not recover completely)
230 x .05 = 11.5 (estimated number of chronic carriers)
11.5 x .25= 2.875 (number of deaths prevented over 20-year span)
So the estimated number of deaths from hepatitis B infection among U.S. children and infants across the first 20 years of mass vaccination of infants is approximately THREE.
Is the vaccine worth it?
A quick search of the VAERS (Vaccine Adverse Events Reporting System) database gives us the answer to that question.
I searched for deaths from Hepatitis B vaccine in children under the age of 15 years.
Here is what I found:
1,237 deaths, with 1,206 (97.5%) deaths in children under the age of 3 years.
1,022 deaths in children under six months of age.
Note: I first looked at the VAERS numbers in February 2012 while researching for another article. The VAERS search in February 2012 indicated there had been 629 deaths in children under six months of age (reported to VAERS). When I researched for the first iteration of this article (June 2, 2014), the VAERS database contained 196 more reports for deaths of infants under the age of six months than the number reported for that same cohort just 27 months prior. That works out to an average of 7.26 deaths per month. If these numbers are correct, that means that in two weeks’ time, more infants were killed by the vaccine than the number of lives (in children aged 0-14 years) potentially saved by the vaccine during the first 20 years of mass administration.
VAERS has been in existence since 1990.
The first four deaths from Hepatitis B vaccine were reported in 1991, when coverage for the vaccine was very low.
The CDC indicates that in 1992, only 16% of infants in the U.S. were vaccinated and during that year there were 13 deaths reported to VAERS.
In the first five years after the Hepatitis B vaccine was recommended for administration to all infants in the U.S., the vaccine killed AT LEAST 235 children. There is a problem with calculating the actual death toll from the Hepatitis B vaccine because even though the 1986 VICP law requires physicians to report suspected adverse events to vaccines, they aren’t doing it. It is estimated that less than 1% of even the most serious adverse vaccine reactions is reported to VAERS.
When my own daughter was seriously injured by a Tdap vaccine in 2010, I told everyone from the ambulance driver to the administering physician, to the doctors and nurses at the hospital, “This is a vaccine reaction and I want it reported to VAERS.” Seven months later, after hearing nothing from anyone in the way of a follow-up, I searched the database and found nothing. I called HHS and asked what was going on. I asked, “Isn’t it legally required for them to report?” (yes). I explained that I had told EVERYONE involved, and none of them had reported. I asked, “Who is responsible for reporting?” I was told that BOTH the doctor who administered the shot and the doctor who treated her at the hospital should have reported. I asked, “So, what is the penalty for not reporting?” I was told, “There is no penalty.” My response: “If there is no penalty for not reporting, it’s not a requirement, it’s just a suggestion.”
When physicians are not really required to report adverse reactions, how can we have the information we need in order to make accurate decisions about the risks vs. benefits of vaccines?
The makers of the hepatitis B vaccine admit they have no idea if the vaccine will impair fertility in those who receive it. They also admit they have no idea how long any immunity from vaccination will last. (Engerix) (Recombivax)
The makers of the hepatitis B vaccine report that it has been tested along with DTP, Oral Polio, MMR-II, Haemophilus B vaccine, Inactivated Polio Vaccine, DTaP or Varicella vaccine. Note the use of the word “OR” – not “AND.” (Engerix) (Recombivax)
Yet, when infants are injected according to the CDC’s Schedule, they frequently receive ALL of the following vaccines:
Hepatitis B, Rotavirus, DTaP, Hib, Pneumococcal vaccine, IPV, Influenza, and now, COVID-19.
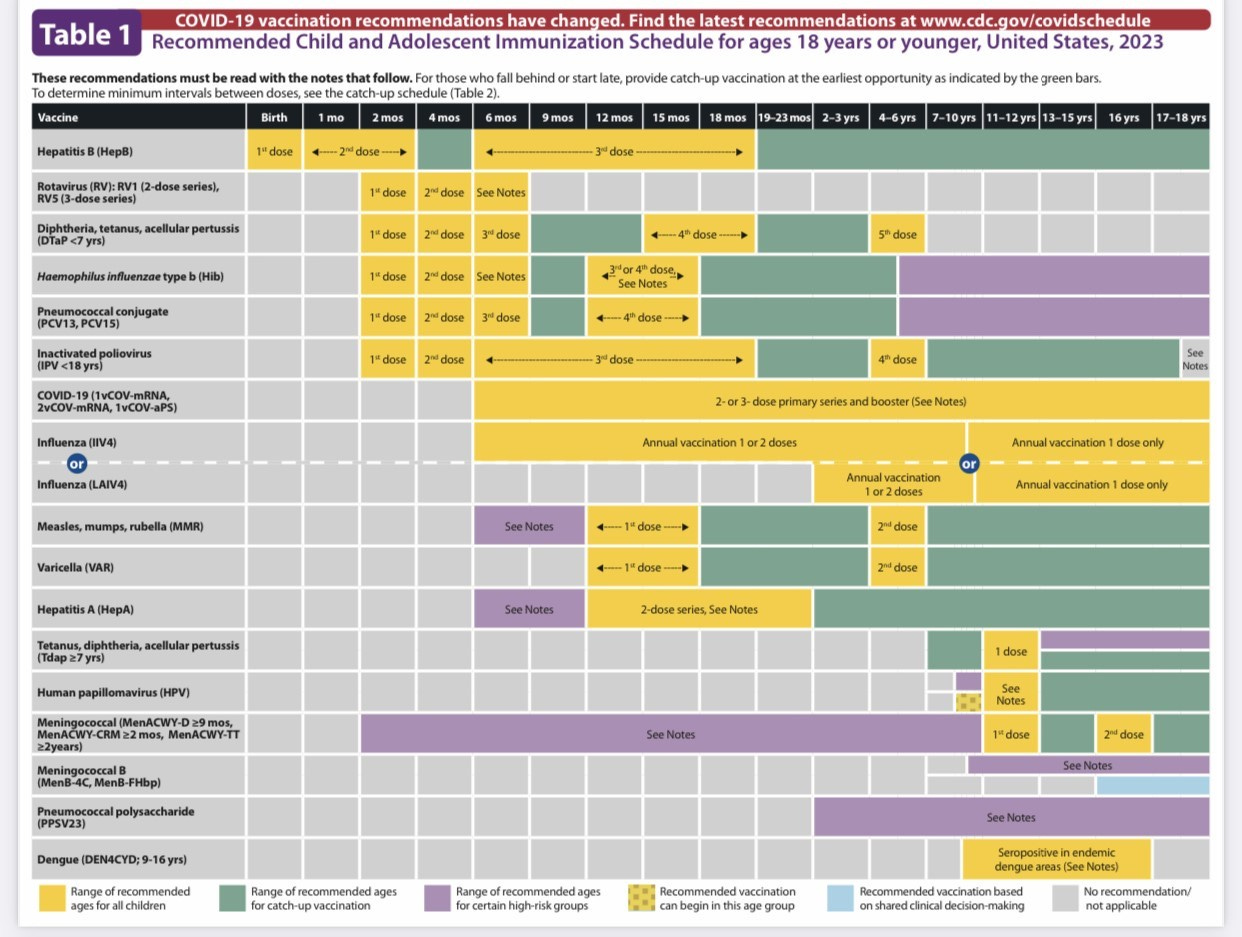
Source: Recommended Child and Adolescent Immunization Schedule, United States, 2023 (cdc.gov)
This is clearly experimental and has not been studied for either safety or efficacy.
According to the Nuremberg Code, which was established in response to the horrific war crimes committed against prisoners during World War II, there are a number of rules that must be obeyed with regard to the performance of medical experiments on human beings.
The rules set forth in The Nuremberg Code dictate, among other things, that
“The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.” (citation)
Clearly, when the number of deaths from the hepatitis B vaccine is at least many hundreds of times the number of deaths that could be expected in children under 15 as a result of hepatitis B infection, we can say with certainty that this is in violation of the Nuremberg Code.
Is this a case where we can say with confidence “When we KNOW better, we DO better?”
For many parents I know, the above quote from Maya Angelou is the case, particularly for those of us who have experienced the trauma of losing a child as a result of vaccine-injury. When our children are harmed by vaccines, many of us turn our efforts toward trying to figure out why. We research and we do everything we can to learn from our mistakes, in hopes of preventing further harm to our children.
The problem is, the same cannot be said for the United States Government, and for the officials within the government who are charged with making decisions about requirements for vaccination of U.S. children.
Documents from the Institute of Medicine, published in 1994, indicate that there have been serious concerns about the research regarding vaccine safety for nearly two decades. The following is from the conclusions of the IOM report:
“The lack of adequate data regarding many of the adverse events under study was of major concern to the committee… the committee encountered many gaps and limitations in knowledge bearing directly or indirectly on the safety of vaccines. These include inadequate understanding of the biologic mechanisms underlying adverse events following natural infection or immunization, insufficient or inconsistent information from case reports and case series, inadequate size or length of follow-up of many population-based epidemiologic studies…”
Documentation of debate that took place at the 2000 Simpsonwood Conference, between officials from the CDC, FDA, and vaccine-industry experts reveals there were serious concerns more than twenty years ago about the effects of mercury and aluminum, and about the number of vaccine antigens injected into infants when they are vaccinated according to the CDC’s Schedule. Rather than coming forward with this information and informing parents and the public, the information was kept secret and was only made known after the documents were obtained through the Freedom of Information Act. (citation)
Despite these very significant concerns, including those related to neurological damage, learning disabilities, autism and even death, the officials in the U.S. government refused to act and refused to inform the public of the dangers, opting instead to not only keep the schedule as it was, but to continue to ADD new vaccines.
This is CLEARLY a case where we can say it is NOT TRUE that “When THEY know better, they do better.”
But perhaps we should not expect “THEM” to do better. After-all, we are not talking about parents, we are talking about government entities. The difference between the huge machines that characterize the U.S. government and those of us who are parents is that machines do not have children. Machines are not parents. Machines do not share the same rights and responsibilities to infants and children as the rights and responsibilities of parents.
Parents are the ones who must make medical decisions for their own, individual children. This is true when we are talking about things like riding a four-wheeler or skateboard, and it is true when we are talking about giving consent for complex medical procedures, including vaccinations – especially when they are given in combinations that have never been studied.
It would be ideal if we could count on the government to care about the well-being of our children.
It would be ideal if we could count on the government to learn from the deaths of thousands of children from the hepatitis B vaccine, and to change the vaccination policy to prevent future, needless deaths.
History has shown us that if we expect these things from the government, we are setting ourselves up for disappointment, and we are putting our children in harm’s way.
Ultimately, our children are our responsibility. It is our responsibility to care for them and to protect them. That responsibility extends beyond our own homes and our own neighborhoods. Unfortunately, when it comes to vaccines, our responsibility to protect our children includes protecting them from the machines that do not have the capacity to Do BETTER, even when they KNOW BETTER.