


Tedros, WHO, COVID, Self-Spreading Vaccines, and MTHFR
It's not paranoia if they're really out to get you.

At last month’s World Health Assembly’s meeting in Geneva, WHO Director-General, Tedros Adhanom Ghebreyesus declared war on anyone who questions the safety or necessity of vaccines. Here is the text of a speech he delivered on May 29, 2024:
Celebrating 50 years of Immunization Progress: Honoring Achievements, Embracing Innovation, and Envisioning the Future
29 May 2024
Honourable Minister Budi Gunadi Sadikin,
Honourable Minister Khumbize Chiponda,
Excellencies, Honourable Ministers, dear colleagues and friends,
Thank you, Honourable Ministers, and all of you for joining us this evening.
Vaccines are among the most powerful inventions in history.
Thanks to vaccines, smallpox has been eradicated, polio is on the brink, and many once-feared diseases can now be easily prevented, including measles, cervical cancer, yellow fever, pneumonia and diarrhoea.
With the recent development of vaccines against diseases like malaria, millions of more lives can be saved.
But only 50 years ago, in 1974, fewer than 5% of infants globally were vaccinated.
Millions died of diseases such as measles, polio and diphtheria.
That was the year WHO launched the Expanded Programme on Immunization, or EPI.
Today, about 84% of the world’s children have received three doses of the vaccine against diphtheria, tetanus and pertussis – diseases which were once a death sentence.
With smallpox, the world showed that through unprecedented global cooperation, vaccines could actually eradicate some diseases.
Building on that success, EPI supported countries to establish standardized vaccination programmes against smallpox and six other diseases: diphtheria, measles, pertussis, polio, tetanus and tuberculosis.
In the five decades since, every country has established an immunization programme, often with support from WHO, UNICEF, and our partners.
Now called the Essential Programme of Immunization, these programmes do far more than ever imagined 50 years ago.
The EPI programme helps millions of children, adolescents and adults access vaccines against 30 diseases.
A new study led by WHO estimates that the EPI has saved at least 154 million lives since 1974 – an average of more than 8,000 lives saved a day, for the past 50 years.
Thanks to immunization, a child born today is 40% more likely to see their first birthday than a child born 50 years ago.
This progress results from partnership – leaders, scientists, civil society, communities and families who have worked together to deliver on the dream of immunization for all. Thank you to all our partners here tonight.
But vaccines don’t deliver themselves. They require a person – and not just any person. So I say thank you to the health and care workers all over the world who ensure the promise of vaccines is realised.
Earlier today, the World Health Assembly approved the 14th General Programme of Work – GPW14 – our global health strategy for the next four years.
Today we also launched the new WHO Investment Case, which estimates that if fully funded, GPW14 could save 40 million lives over the next four years.
One of the main ways we can save those lives is through immunization.
The EPI is one of our best examples of what is possible when we invest in WHO, work in partnership and prioritize health for all.
WHO is committed to working with all of you to realise the power of vaccines for more people.
I would particularly like to acknowledge the very important role that Gavi plays in supporting access to vaccines around the world.
Just as we ask donors to fully fund the GPW, we also ask you to support Gavi’s replenishment later this year.
More than 14 million children in 2022 did not receive a single dose of vaccine. Working together with partners like Gavi and UNICEF, we aim to halve that number by 2030.
Tonight, we celebrate the incredible success of EPI over the past 50 years. It shows what is humanly possible.
With continued research, investment and collaboration, we can save millions more lives in the next 50 years, and beyond.
I thank you.
Here is where you can find the speech on the WHO website.
Here is a video of Tedros giving the second half of the speech. Watch this video from The Canadian Independent, please.
After the completion of his “official” prepared speech, Tedros declared his intent to get “more aggressive” in the WHO’s battle against “anti-vaxxers” and “all the havoc they are creating.” The text of this part of his speech is not included on the WHO website. I wonder why not? Is it possibly because the Director-General does not want his intentions on the record for posterity?
Warning: The rest of this post is going to sound like a conspiracy theory. That’s because it is. I have no solid research to back up what I’m about to say. This is something that has been on my mind off and on for a few years now, ever since it became pretty obvious that the COVID-19 injections are “shedding” and that the spike protein being produced by those who took the shots is being shared with everyone around them, including those of us who intentionally did not take the shots.
My theory timeline starts in January of 2019, when the World Health Organization published its list of Ten Threats to Global Public Health, including “Vaccine Hesitancy” among its targets for elimination. In doing so, WHO at least appeared to be setting its sights on eliminating anti-vaxxers with the same zeal as if it were going after Ebola, pandemic influenza, anti-microbial resistance, and Dengue Fever.
I recall when I first heard that people who had not been injected were experiencing bleeding problems after being around people who had been recently injected with the mRNA shots.
Facebook post:

It wasn’t long after the deployment of the mRNA shots that we started hearing about the increase in sudden deaths from stroke and heart attack, and the blood clots – all in those who had lined up for the shots. But now, within a very short time after the deployment of the gene-therapy shots, we started hearing about bleeding problems in people who had not taken the injection. All of these things caused my radar to really go off, and I started thinking that the people who were being most affected by the shots and by the shedding were probably people like me. Those of us who carry the MTHFR genetic SNPs. Despite what The CDC will tell you, MTHFR genetic mutations increase the risk of serious vaccine injury. They also increase our risk of recurrent miscarriages, early strokes and heart attacks, phlebitis (blood clots), and DVT (deep vein thrombosis).
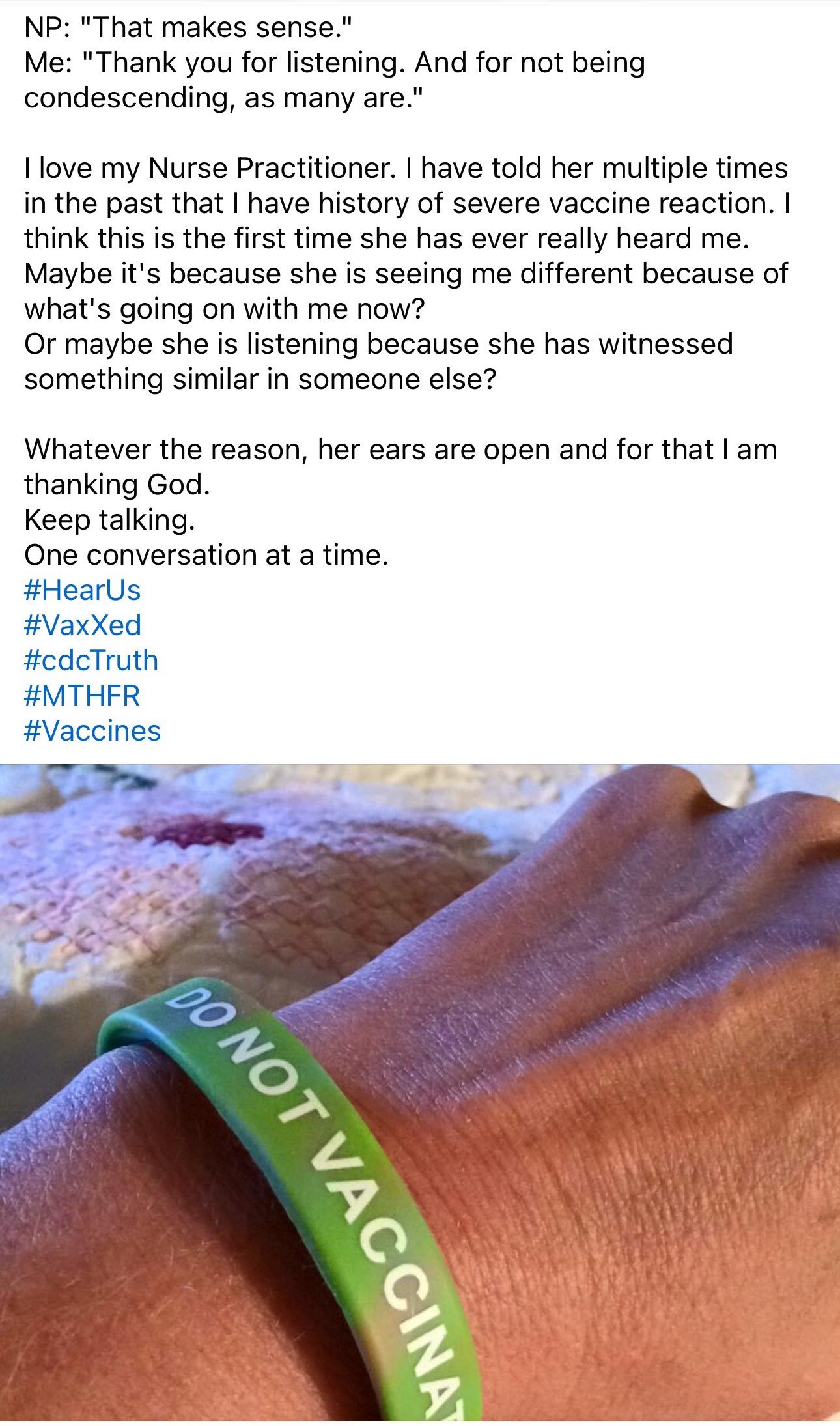
The following three screenshots are from a post I made in 2016, nearly four years before anyone had heard of COVID:
Here is the link to the study mentioned above: Journal04-04a.cdr (jpands.org)
The more I heard about “unvaccinated” people suffering from bleeding and clotting problems after being around those who were jabbed, the more I began to think this was not a coincidence and may have been a primary goal when this “thing” was being created in the lab. In my head, the conversation goes like this:
“Let’s see if we can make this benign virus more infectious and deadly through gain-of-function research, and while we’re at it, let’s see if we can make it target the very people we want to eliminate, since they are one of the top threats to global public health.”
In effect killing two birds with one stone. Or, killing millions of people with one shot, while increasing the chances that those eliminated would be the ones already targeted for reduction by WHO.
Facebook post:
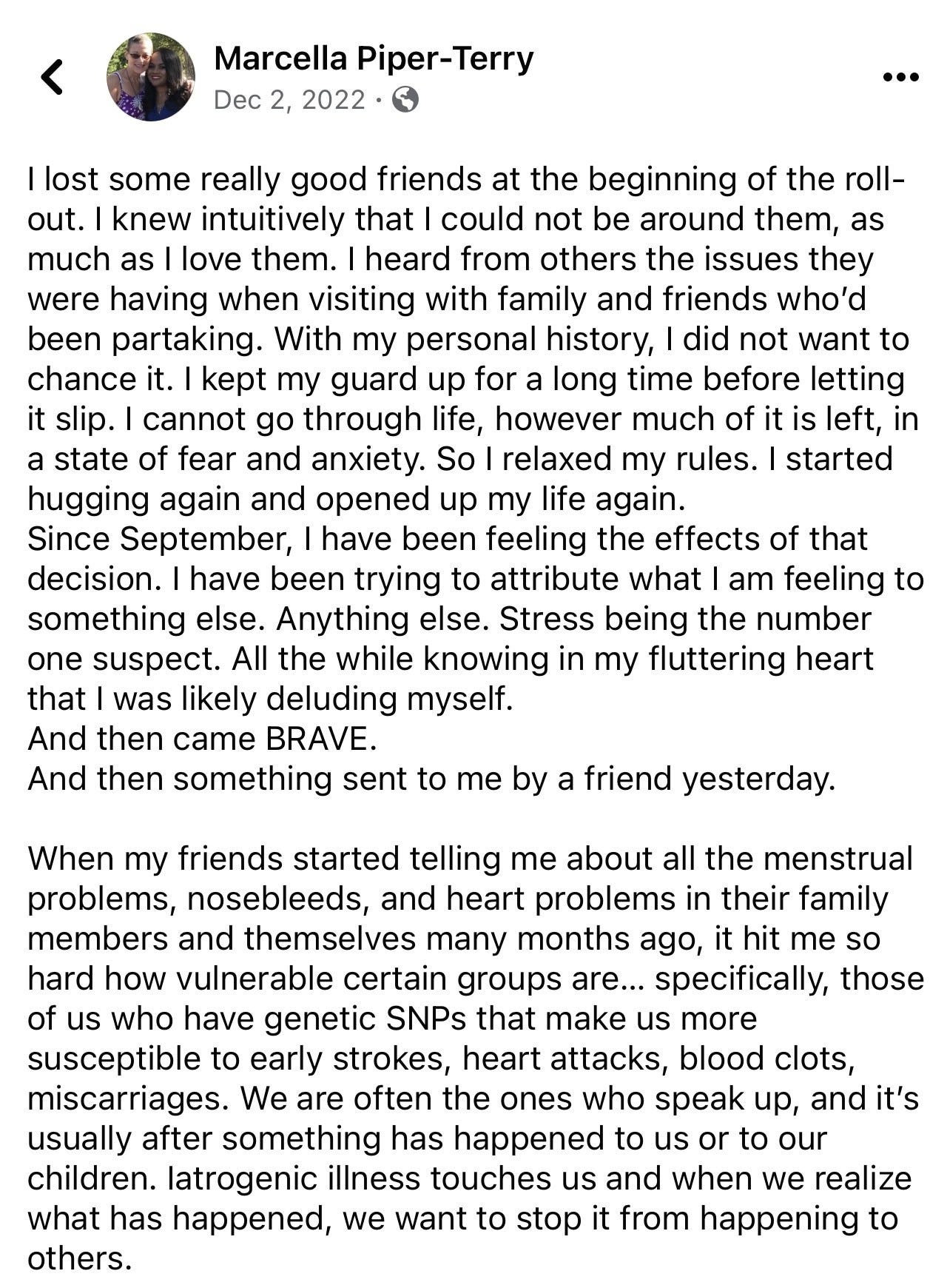
Since December of 2022 and Dr. McCullough’s video on shedding (pictured in the comments of the above screenshot), Dr. Pierre Kory has published a 9-part series on shedding of the mRNA gene therapy shots. Dr. Kory has also teamed up with “A Midwestern Doctor (AMD) and together, they have worked to really compile and organize the evidence, which is summarized here:
OVERVIEW OF THE SCIENCE OF mRNA VACCINE SHEDDING
A quick summary of the scientific case we have built is as follows:
1. COVID mRNA “vaccines” are gene therapy products as defined in the FDA’s 2015 document on Gene Product Shedding Studies.
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
2. The FDA document defines shedding of gene therapy products as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
3. All other gene therapy products on the market list shedding as a risk in their insert (Luxterna, Roctavian, Zolgensma) and shed from 7 days to 6 months
4. Pfizer was aware of the risks of shedding and specifically stated in their protocol that study investigators collect reports of environmental shedding events (trial protocol p. 67)
5. The mRNA vaccines are also defined as “nanoparticle technology” which can be synthetic or biologic (i.e. exosomes). Synthetic nanoparticles distribute widely in the body and easily traverse numerous physiologic barriers (most notably can be inhaled and absorbed by the lungs)
6. mRNA gene therapy products (spike protein) have then been found in circulating exosomes for up to 187 days after vaccination (after which study was stopped). Note that exosomes can be easily transmitted via the breath, and absorbed into the lungs of those nearby.
7. Data from Dr. Burkhart’s autopsy series (and cases reports) show widely disseminated spike in numerous organs after vaccination
8. Breast Milk shedding: Numerous animal and human studies report mRNA and/or spike protein in breast milk after vaccination.
a. Pfizer post-surveillance data contain numerous reports of breast fed babies suffering anaphylaxis, strokes, seizures, and respiratory arrest after a feeding.
9. Placental shedding - synthetic nanoparticle and exosomes readily cross the placental barrier. A recent paper found both mRNA and spike protein within the placentas of two mothers vaccinated shortly before delivery.
a. The CDC recommends investigation into any VAERS adverse event with a “Proportional Reporting Ratio (PRR) compared to the influenza vaccine which is greater than 2. There are now 11 pregnancy and fetal adverse effects reported to VAERS with PRR’s ranging from 3 to 300.
10. Person-to-Person Shedding - one study reported unvaccinated children of vaccinated parents developed antibodies to spike protein. Another study found that excess mortality of unvaccinated children in the USA and Europe increased during the first 18 weeks after the adult vaccination campaign rollout (i..e at a time when children were NOT being vaccinated).
a. Two groups of researchers, one including myself and AMD put out a public call for shedding reports. We now have over 1,000 reports which are:
i. repeatable and predictable
ii. evenly split between people who reported a cluster of symptoms vs. a single symptom
iii. submitted by people who reported symptoms that matched what many others reported
11. Patterns Of Shedding Reported:
a. Primary: when someone gets ill from being around a vaccinated person (e.g. vaccinated parents making their unvaccinated children ill)
b. Secondary: when someone gets ill from being around a person who was recently around vaccinated people, (e.g., children being shed upon and then affecting parents after coming back home from school).
12. Susceptible Patients
a. Sensitivity to shedding varies immensely and generally only affects environmentally or physiologically sensitive people
b. Symptoms resemble what is seen in other spike protein-induced syndromes (e.g., long COVID/long Vax).
c. Patients develop similar symptoms after a shedding exposure, particularly after a “strong” shedding exposure
d. Many patients reported repeated shedding symptoms emerge after the same exposure
13. Characteristics of “Shedders”
a. dramatically more likely to shed soon after vaccination (the very sensitive claim they are susceptible far beyond a 2-4 week period)
b. shedding events (in the same location) are the most frequent and severe immediately following a new booster rollout
c. young and healthy people tend to shed more frequently
d. shedding greatly varies by the individual (e.g., “I react to specific people I see at church”).
14. Most Common Symptoms: Menstrual abnormalities (by far), Decidual Cast shedding, Headaches, Tinnitus, Nosebleeds, Painless, inexplicable bruising, Dizziness, Brain Fog/Malaise, Skin Rashes
15. Less Common Symptoms: Atrial Fibrillation/palpitations, Muscle Pain, Seizures, Peripheral Neuropathy, Insomnia, Hair Loss, Swollen Lymph Nodes, Severe abdominal pain, Sinus Pressure/Copious discharge, Vision/Eye Problems
Rare Symptoms: Stroke, Blood clots, Severe heart injuries in children, Polymyalgia Rheumatica, Death, Cancers, Sensory Neuropathy, Anxiety
So, we know from Dr. Kory’s and AMD’s research that it was known before deploying the mRNA gene therapy shot that it would act as a “self-spreading vaccine.” Going a bit further in my conspiracy theory, I believe this may have been intentional and if it was, I believe it was done to take away our ability to “opt-out.” I also believe this may be part of why the J&J shot and the AstraZeneca shot were either not approved or quickly phased out. They don’t have the same effect on those of us who were attempting to protect ourselves from vaccine injury or vaccine-induced death by adopting the stance of “Just Say NO.”
Facebook post:
You may think this is completely unbelievable. Our collective world governments would never go along with this. Yeah. I used to think the same things.
It was 2016 when I first became aware of research that is exploring “self-disseminating vaccines.”
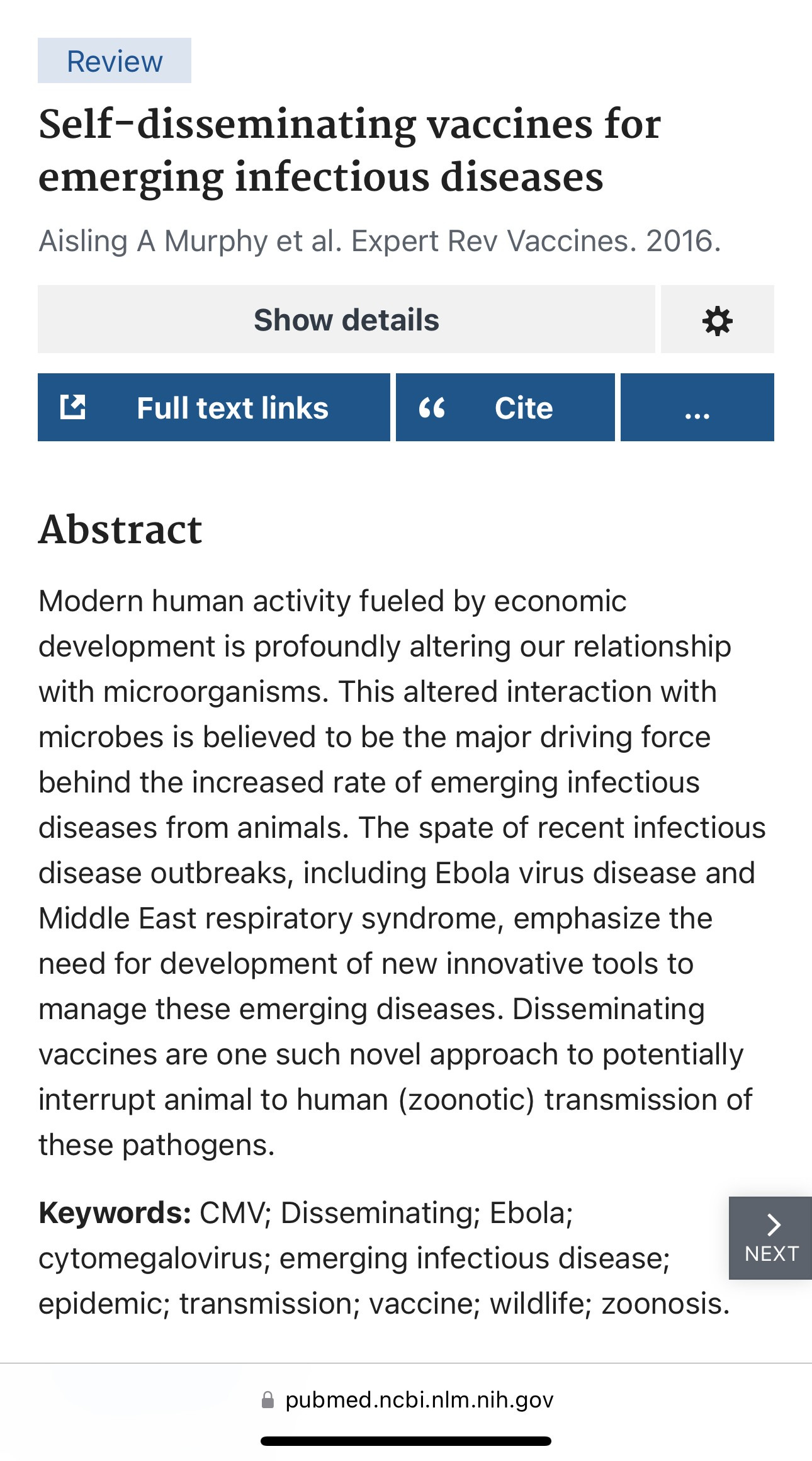
The limited information published online about “self-disseminating vaccines” discusses using these self-spreading vaccines in wildlife populations. The way it’s supposed to work is that you can vaccinate a small percentage of the population, and they will then basically vaccinate the rest of the population, just by coming into contact with them.
I can’t find any stated intentions to use this kind of vaccine technology on humans. The part of me that no longer trusts our government scientists at NIAID or those at The WHO has a hard time believing that they would never use that technology against humans without our consent. They clearly knew that the mRNA gene therapy shots “shed” from person-to-person before they deployed the “vaccines” on the population of the world. They didn’t tell us about that.
Is there any evidence that might suggest that people with MTHFR genetic mutations might have been a target when they were developing the “virus” and their gene therapy shots? I guess I wouldn’t call it “evidence” in the true sense of the word, but there is now some research indicating that those of us with MTHFR genetic mutations fare worse when it comes to both COVID infections and the COVID shots.
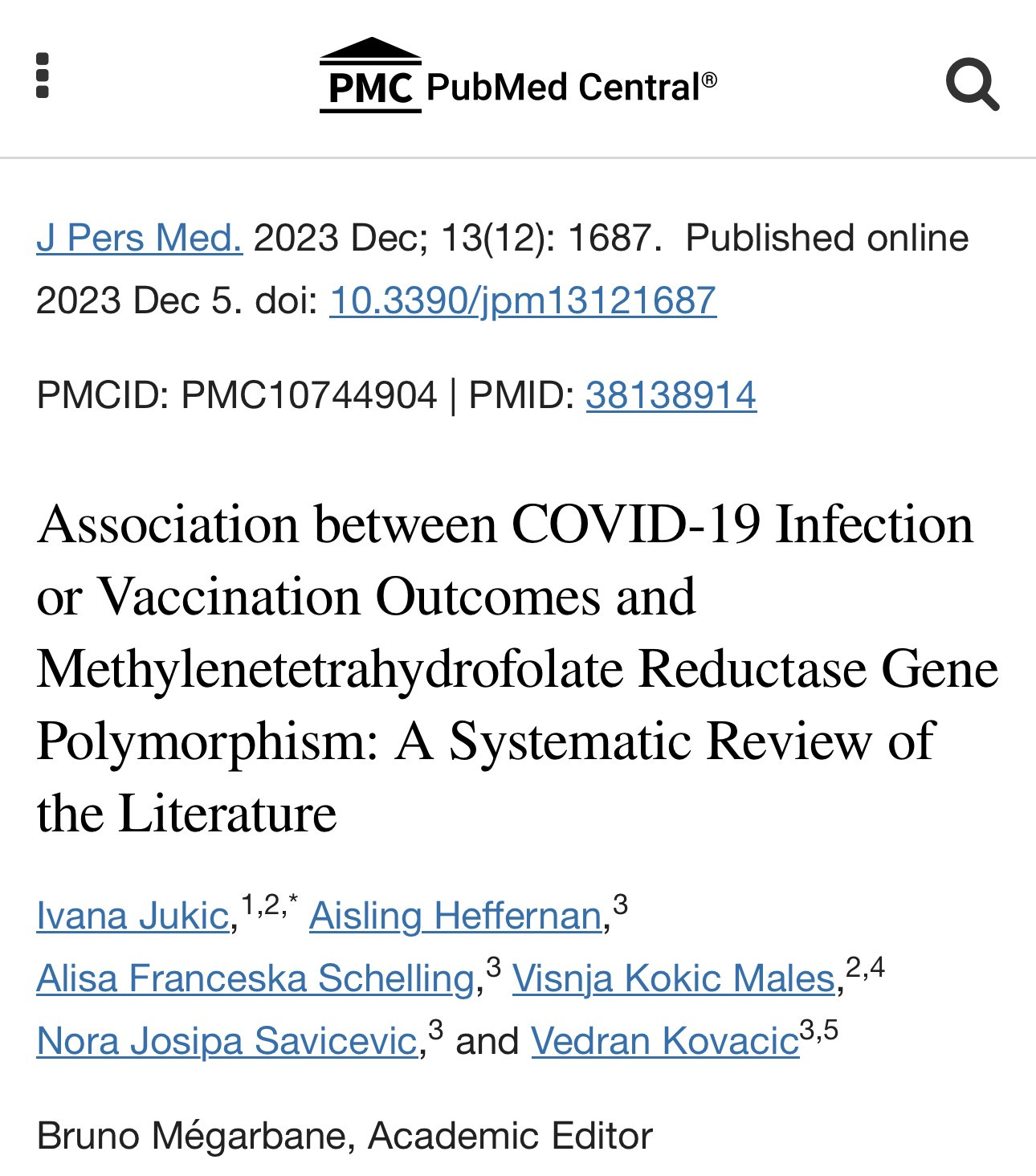
From the study:
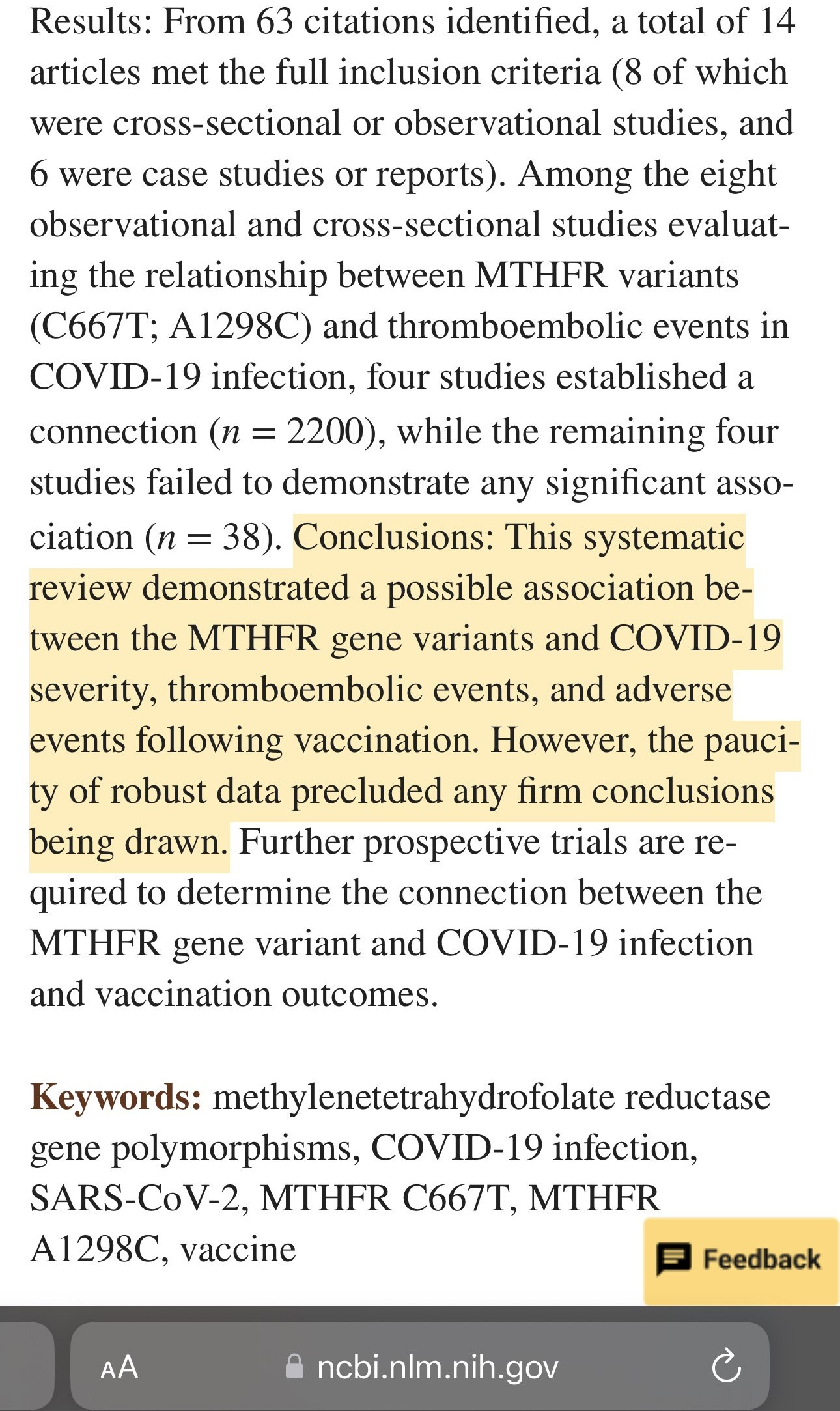
The authors of the above review note that among the 8 studies they included in their analysis, 4 showed an association and 4 did not. Notice the difference in the numbers between those that did (N=2200) vs those that did not (N=38). This is not at all surprising to anyone who understands statistics. The smaller your number (of subjects), the less likely you are to find significance.
I don’t know if any of this was intentional. Because I generally like to rely on things that are verifiable, I try to stay away from hypothesizing out loud when I know I cannot verify. It’s just that so much of what has happened over the last four years has been based on lies and profit, and the entire scientific process has been tossed aside in the name of compliance and control. With The WHO’s goals of trying to remove our individual freedoms and attempting to take over the response of ALL nations around the world when the next “pandemic” emergency is declared, coupled with Tedros’ promise of increased aggression against those of us who refuse to comply, the future does not look good.
It is definitely not the time to let our guard down. It is the time to do all we can to protect ourselves by working to attain our best state of wellness, and to do all we can to stay healthy. If you haven’t been following Dr. McCullough’s recommendations for degradation of spike protein, I highly recommend doing so. You can find that information here.
Be well and stay vigilant, friends.
an interesting connection i found while researching an article i wrote - many who have MTHFR ALSO have an issue with Biotin - they tend to have Low Functioning Biotinidase. Biotin issues also have direct correlation to hemotological issues along with all manner disease, cancer and Neurological issues. On top of this - vax and meds are bioengineered to be delivered via the Biotin pathways in the body and can then corrupt Biotin function which in turn can corrupt B12 functions. I explain all of this in detail in an article I wrote in 2020 BEFORE the latest VX. I also explain why and how this can directly connect to induced autism. My article is entitled Neurological and Autoimmune Reactions and Diseases : Vaccine and Medication Side Effects - The Biotin/B12 Connection. This is the direct link to it if you care to read. https://beingthankfulfor.com/2020/04/11/neurological-and-autoimmune-reactions-and-diseases-vaccine-and-medication-side-effects-the-biotin-b12-connection/
Even if you don't have MTHFR this info about Glutathione, Antioxidants and....is important.
https://gregeldefonso.substack.com/p/httpswwwlivingwithmthfrorggenetic