


We are Anti-Vaccine Wackos: It's just what we do.

If you have been labeled an “anti-vaxxer,” you may not be thrilled with me also referring to you/us as a “wacko.” I did this intentionally. We are so vilified in the press, with the obvious intent to turn us into a nation of “us” vs. “them.” Nobody wants to be so unpopular. Nobody wants to be saddled with such a negative label. But we are. And one of the main themes of this campaign against anyone who dares to speak out is that we are tin-foil wearing wackos who can’t read science and who deserve to be diagnosed with a DSM-V label for our “obvious mental illness.” Well, here’s a news flash: Doubting and questioning are the basis of science. And it doesn’t take a PhD to figure out that something has been going terribly wrong for a long time when it comes to childhood vaccines. My use of the word “wacko” is my attempt to take charge of the narrative. Using it myself defuses any power it may have had otherwise.
Many people who have been referred to as “anti-vaxxers” are actually ex-vaxxers. We vaccinated our children exactly as we were told to do by our pediatricians and family doctors. We followed the CDC Childhood Schedule. Until something bad happened. For those who have recently been labeled “anti-vaxxer” due to hesitancy, questioning, or being vocal about their own reactions to COVID-19 shots, my “welcome to the club” speech is tempered with sadness. The one thing we have not ever wanted was for the size of our club to grow, and certainly not in the numbers we have seen over the last two years.
If there is a positive thing about the whole COVID-19 debacle, it has to be that so many people who were previously unaware of the problems in our nation’s public health system are no longer following blindly and just doing as they are told. The process of seeing how the sausage is made has led to more parents than ever questioning the childhood vaccination schedule, and that can only be a good thing for the future of American children.
Probably the biggest issue, as it relates to autism and other neurodevelopmental, immunological, gastrointestinal disorders is the overwhelming number and concentration in the ever-growing childhood schedule.
In 1983, this was the CDC’s Childhood vaccine schedule:
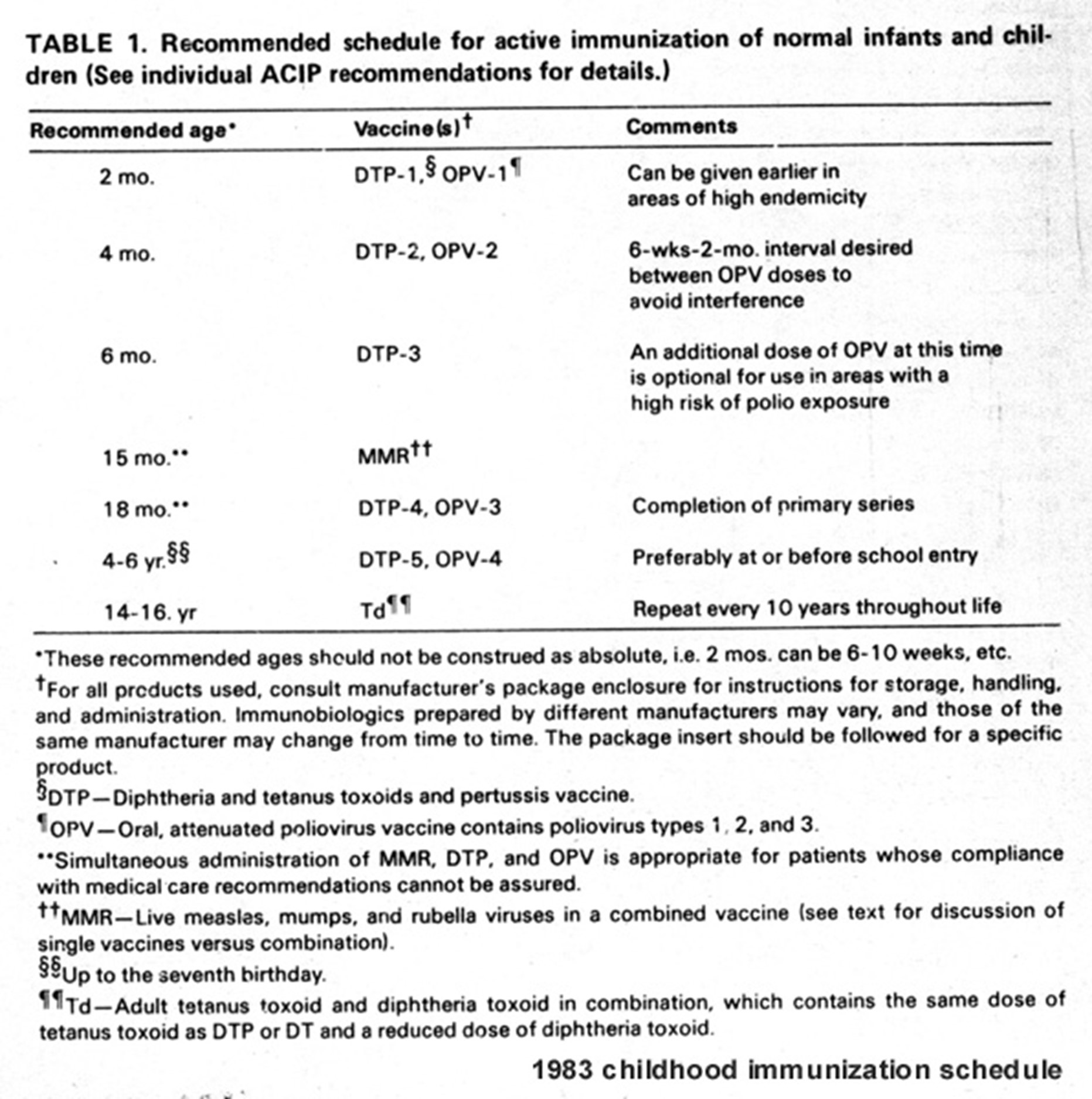
It is important to note that in the mid-1980s, the rate of autism in the United States was estimated to be 1 in 10,000 children. As we can see from the 1983 schedule, at that time, American children who were vaccinated according to “The Schedule” received a TOTAL of 11 doses of 7 vaccines, beginning at 2 months of age, with the last recommended vaccine (a booster for tetanus and diphtheria) given between 14 and 16 years.
In the 1980s there were no recommended vaccines for pregnant women, so babies were not receiving vaccines in utero. In their first eighteen months, babies received a total of 8 doses of 7 vaccines: 3 doses of diphtheria, tetanus, and pertussis, three doses of the oral polio vaccine, and 1 dose of measles, mumps, and rubella. (Just a note here… DTP and MMR are each only one injection, but there are three vaccines in each injection.)
During the 1970s and 1980s, vaccine makers were being sued as a result of injuries and deaths which were largely attributed to the whole cell pertussis component of the DTP shot. The vaccine industry basically blackmailed the United States government, threatening to stop making vaccines altogether unless they were protected from liability. On November 14, 1986, then President Ronald Reagan signed into law the National Vaccine Injury Compensation Program (NVICP), which gave vaccine makers protection against lawsuits when their products injure or kill. Since that time, a seventy-five-cent tax on each vaccine administered goes into a fund which is supposed to help pay for vaccine-injuries and deaths. The way it was supposed to work is that when a child is injured or killed, the parents can sue the government (not the vaccine maker) and obtain financial assistance/compensation. A “Vaccine Court” was created. There are a lot of problems with the program, including the fact that it is heavily weighted against families/victims. It is estimated that approximately 1 out of 1,000 people who file a claim prevails in “Vaccine Court.” Since the establishment of “Vaccine Court” in 1989, more than $5 Billion has been awarded to successful plaintiffs. Not one penny of that has come from the pharmaceutical industry. It’s taxpayer money.
Part of the 1986 Law provided that as long as a vaccine was part of the CDC’s Childhood Schedule, the manufacturers could not be sued. So, getting their new shots added to the Childhood Schedule is a priority for vaccine makers. Once those shots are on “The Schedule,” there is zero risk to the makers. For anyone who has been wondering, this is a primary reason why the “COVID emergency” lasted as long as it did. The vaccine makers had to get their products on The Childhood Schedule in order to protect them from any future liability that was not covered under the pandemic regulations. As soon as that was accomplished, “the emergency” was officially declared over. Once a shot is added to The Childhood Schedule, there is zero incentive for them to make their products safer, since they have no consequences if they manufacture products that disable and kill children. Think about that for a moment. Vaccines are the only product for which the United States government mandates their use, while simultaneously refusing to provide protection when those products cause injuries and deaths.
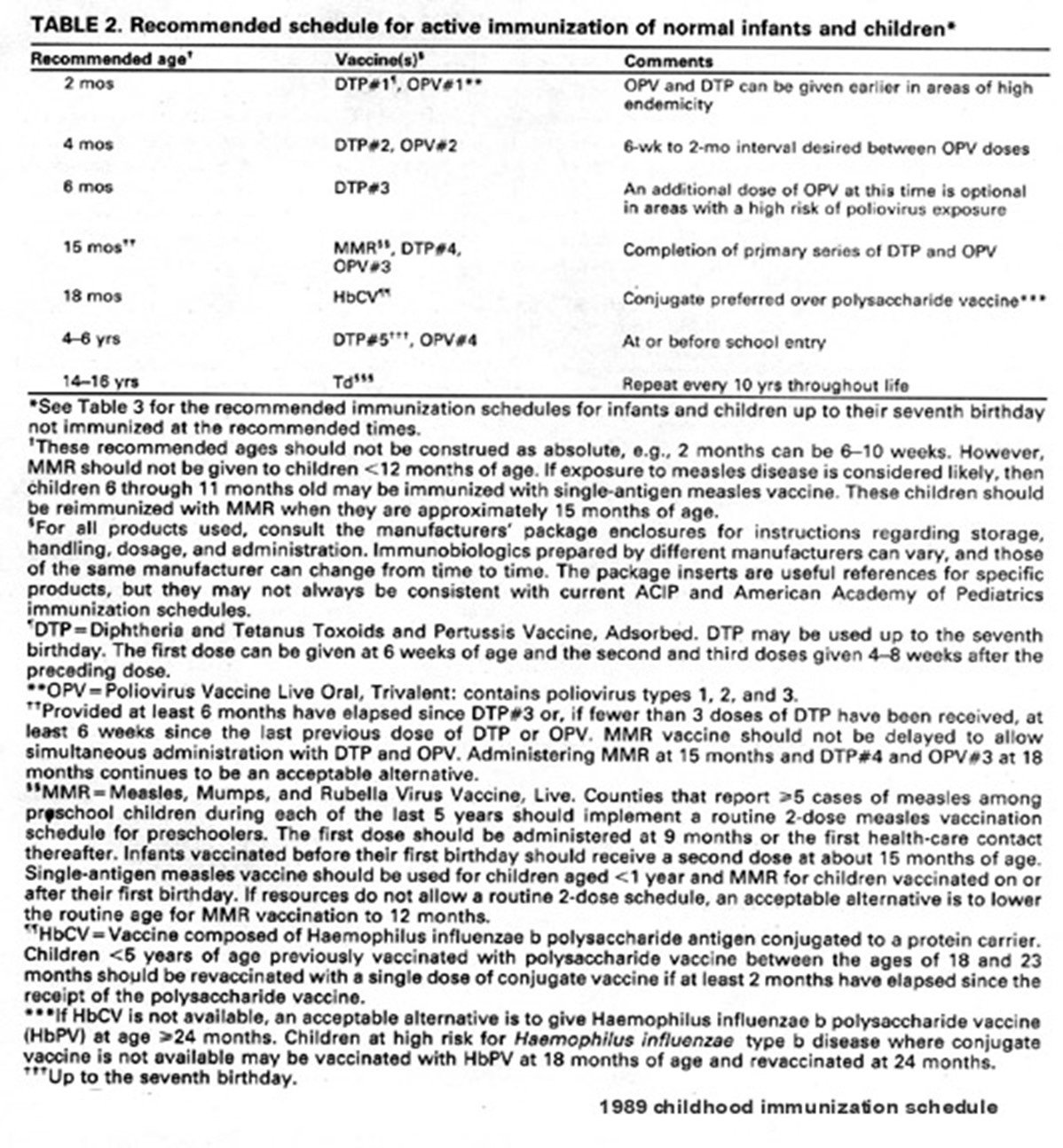
So, what happened after the passage of the 1986 Law? Our children became cash-cows for the pharmaceutical industry and the Childhood Schedule exploded. It started slowly, with a change to the schedule in 1989, when a single dose of Haemophilus B Influenza vaccine was added at 18 months.
The explosion of sick kids began in the early 1990s. Looking at the difference in the vaccine schedules, we can see that this time frame coincides with the addition of the Hepatitis B vaccine. Recent studies have shown that any immunity conferred by the hep B vaccine series is gone within 2-5 years. Another recent study found that boys who were vaccinated against Hepatitis B were three times more likely to develop autism than boys who were not vaccinated against Hepatitis B. Hep B is a sexually transmitted disease. Infants and toddlers usually aren’t out running around having sex, so there is no justification in giving this vaccine.
The Hepatitis B vaccine was licensed in 1981 and during the 1980s it was recommended for adults who were at high risk of contracting hepatitis B through lifestyle choices (promiscuous sex or IV drug use) or those whose occupations placed them at risk of coming in contact with the blood of an infected person (healthcare workers, prison guards). Vaccine uptake by those “high risk” adult groups was not up to the makers’ expectations. They couldn’t get the adults to take the shot, so they decided to just get everyone when they could - in infancy. (Note the parallels here with the COVID-19 shot, which was added to the schedule, recommending it for ALL infants and children, despite the fact that children have a 0% death rate from COVID.)
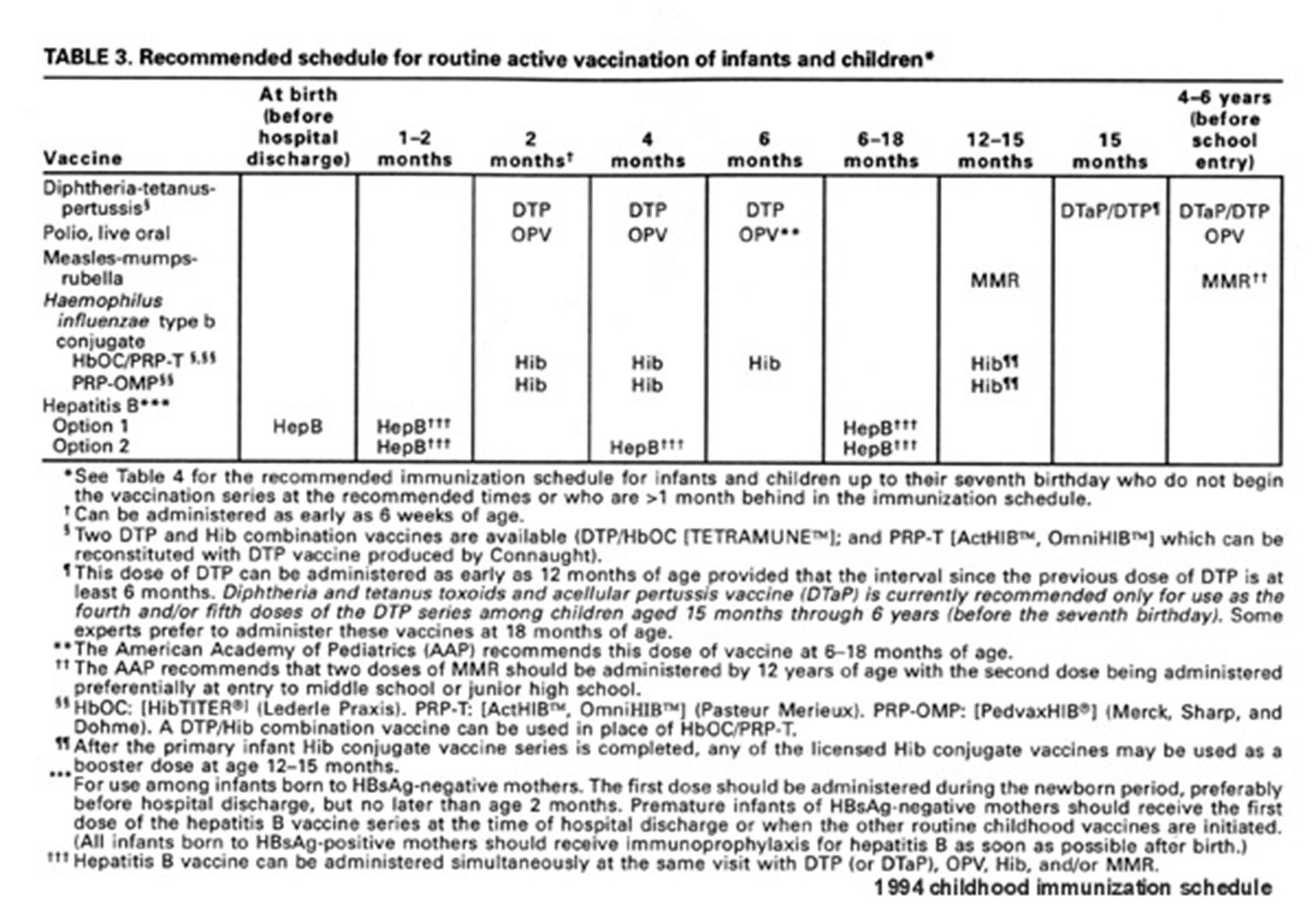
In the early 1990s, the hepatitis B vaccine was recommended for “at risk” infants - those whose mothers were positive for the virus. In 1994, it was added to the Childhood Schedule, with a three-shot series, beginning within 12 hours of birth. The 1994 schedule also included new recommendations for Haemophilus B Influenza (Hib). Previously recommended as a single vaccine, Hib was now also a three-shot series. The 1994 Childhood Schedule also added a second dose of the MMR vaccine, to be given as a booster dose between 4-6 years of age. The second dose of MMR was added because it was determined that approximately 10% of people did not develop any sign of immunity after the first dose. So, instead of taking steps to figure out who those people were, and adding a second dose for them, the blanket recommendation was to give everyone a second dose, in effect, over-vaccinating 90% of the population of American children.
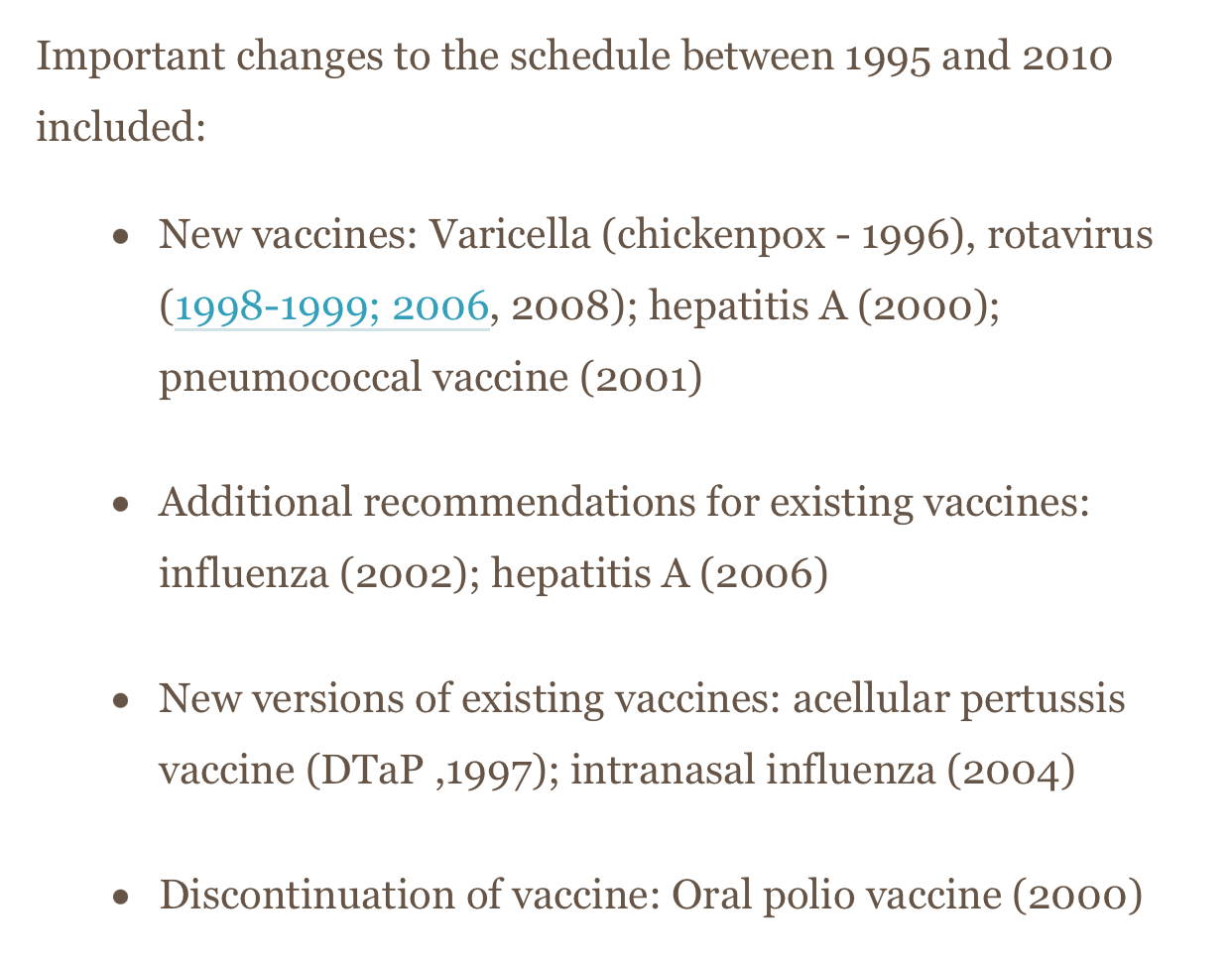
Between 1995 and 2010, there were yearly updates to the Childhood Schedule because new vaccines were being produced and things were changing pretty quickly.
By 2012, this is what the CDC’s Childhood Schedule looked like:
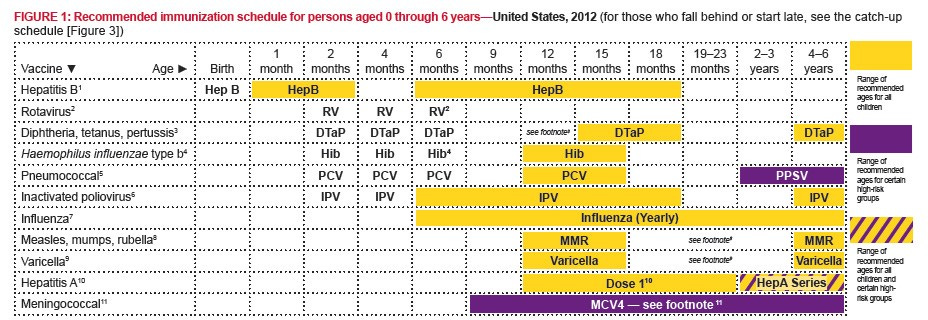
It’s getting increasingly difficult to keep track. The 2012 Schedule includes 43 doses of vaccines for 14 different viral and bacterial infections by kindergarten (age 4-6 years). This number does not include yearly flu shots or meningococcal vaccines, which were only recommended for “certain high-risk groups.” When we add in the yearly flu shots, the number of vaccines administered to children whose parents follow the CDC Schedule (or their pediatrician’s advice) increases to 49 doses of fifteen different vaccines by age five. In 2012, The Schedule recommended thirty-six doses of 14 different vaccines between birth and 18 months of age. Remember, in 1983, children vaccinated according to The Schedule received 8 doses of 7 vaccines by 18 months of age. So between 1983 and 2012, the number of vaccine doses given to infants in their first year and half more than quadrupled and the number of different vaccines for different infections doubled during the same time frame.
You may notice from the schedules posted above that the recommendations were generally for infants and children from birth through age 6 years. That’s because prior to 2005, the industry had not yet fully set their eyes on another group: adolescents. Once they set their sights on pre-teens and teenagers, the Childhood Schedule, which recommends vaccines for children and teenagers from birth until age 18, became so complicated that it now comprises multiple tables and several pages of very small print, just to help doctors and nurses understand what it is they are supposed to be giving and to whom.
This is the primary table for the 2023 CDC Childhood Schedule:
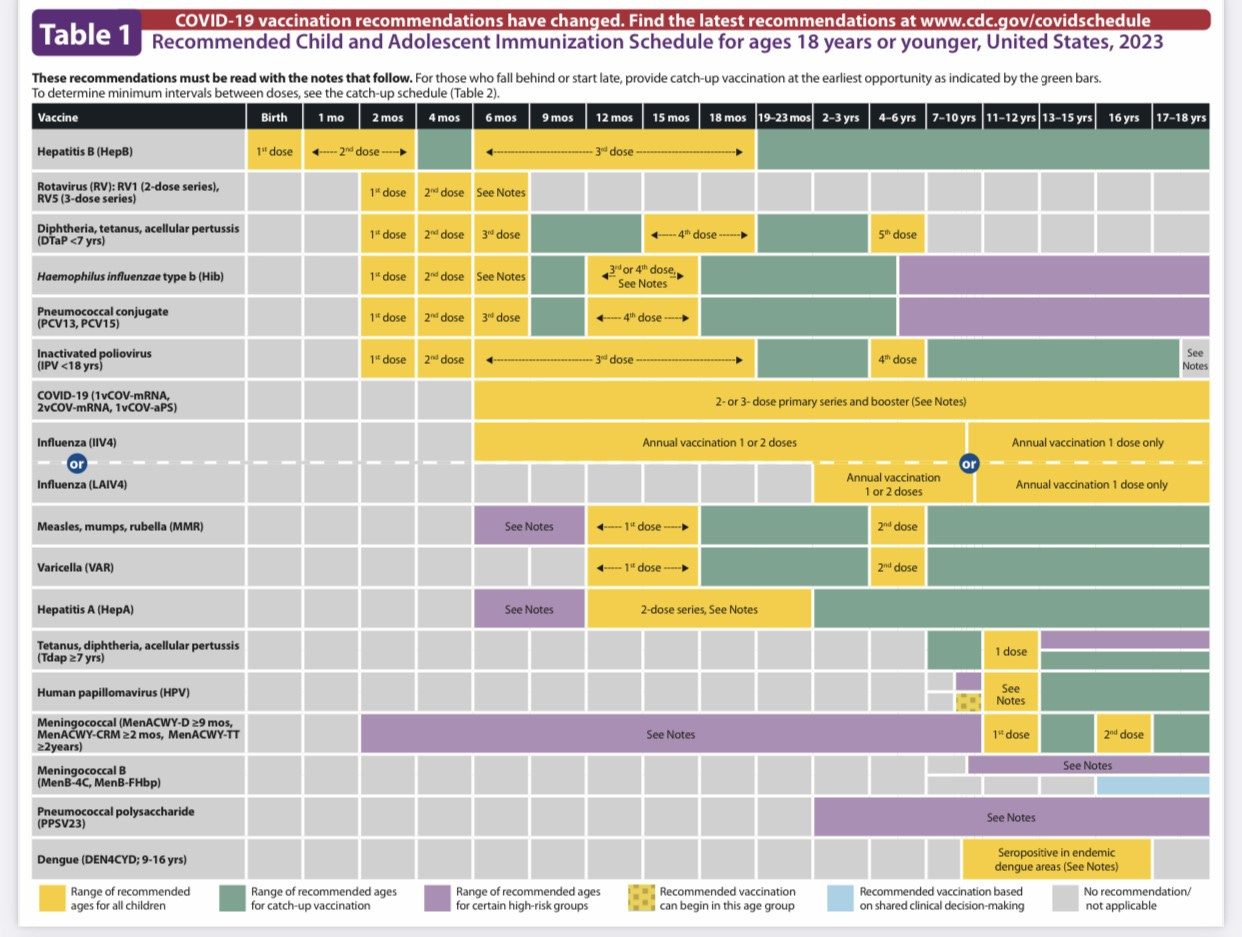
Let’s see if we can simplify this…
Hepatitis B - 3 doses by six months (many children get 4 doses because after the single dose in the hospital, they get a combo shot at their 2-, 4-, and 6-month vaccine appointments (aka “well-baby check-ups”).
Rotavirus - 3 doses by six months
DTaP - 5 doses by age 6 years (diphtheria, tetanus, pertussis)
Hib - 3-4 doses by 15 months
Pneumococcal - 4 doses by 15 months
Inactivated Polio - 4 doses by age 6 years
MMR - 2 doses by age 6 years (measles, mumps, rubella)
Varicella (chickenpox) - 2 doses by age 6 years
Hepatitis A - 2 doses by 23 months
TDap - 1 dose at 11-12 years (tetanus, diphtheria, pertussis)
HPV - 2-3 doses at 9-11 years
Meningococcal (ACWY) - 2 doses by age 16 years
Meningococcus B - 2 doses between 16-18 years
Influenza - yearly, from 6 months to 18 years - 2 doses per year from 6 months to 8 years (16 doses); 1 dose per year from 9 years to 18 years (10 doses); total 26 doses.
COVID-19 - 2 or 3 dose primary series, plus boosters (number of boosters as yet to be determined)
The total I come up with here is between 65 and 70 doses. Things that will influence the final number include whether the infant receives 3 or 4 Hepatitis B vaccines, the age and timing of the HPV vaccine, and whether the initial COVID-19 series is a two or three shot series. I am not including Dengue Fever vaccine in this calculation, since it *should not* affect children living in the continental U.S. - at least not at this time… Some folks will recall that a few years ago, the number of doses was 72. I believe that number was higher because for a while, the CDC was recommending two flu shots per year (one for “seasonal flu” and one for H1N1; they have been combined now into one yearly flu shot).
Of course, if the mother receives vaccines during pregnancy, those need to be counted in the total, since the developing baby will also be exposed to the vaccines (and all of their ingredients). That means we need to add TDap, Influenza, and COVID-19 (2 doses), for another four doses, bringing the total to 69-73 doses.
Counting the vaccines/infections, we have:
Hepatitis B
Rotavirus
Diphtheria
Tetanus
Pertussis
Hemophilus B Influenza
Pneumococcal
Polio
Measles
Mumps
Rubella
Varicella
Hepatitis A
Human Papilloma Virus
Meningococcal (ACWY)
Meningococcal (B)
Influenza
COVID-19
In total, according to the 2023 CDC’s Childhood Schedule (and including vaccines given in utero), children vaccinated according to recommendations receive between 69-73 doses of 18 different vaccines from womb to age 18 years.
If a baby is vaccinated according to The Schedule, that infant receives 20 doses of 10 different vaccines between birth and six months. Adding maternal vaccines given in pregnancy increases the number to 24 doses of 10 different vaccines by six months of age. By 18 months, a child vaccinated according to the 2023 CDC Schedule receives between 32 and 35 doses of 15 different vaccines between birth and 18 months of age. Adding maternal vaccines increases this number to 36-39 doses of 15 vaccines by age 18 months.
Let me restate for emphasis: Infants vaccinated according to the CDC’s 2023 Childhood Schedule receive more vaccines in their first six months of life than children in the 1980s received from birth through age eighteen YEARS.
Remember way back in 1983, when American children received 8 doses of 7 vaccines between 2 months and 18 months of age? And remember that in the 1980s, the rate of autism was estimated to be 1 in 10,000 American children?
According to the CDC, the current rate of autism in American children is 1 in 36. And while they are “absolutely positive vaccines don’t cause autism,” they have no idea what it is that could be causing the increase. They are so sure they refuse to do any studies that might actually reveal the problem. I am reminded here of a quote from Upton Sinclair: It is difficult to get a man to understand something when his livelihood depends on him not understanding it.
While the exploding Childhood Schedule is a significant issue, it is not the only issue at play. The second issue, albeit related to the first, is that current vaccination laws force parents into an “all-or-nothing” stance. In order to claim a religious exemption for school attendance, you have to refuse ALL vaccinations. You can’t pick and choose which make sense for your child. Many physicians will not work with parents who want to exercise caution and spread-out vaccinations. Some physicians “fire” parents from the practice if they even bring up the subject. So, if you ARE concerned about measles, diphtheria, polio, etc. (the “childhood diseases” everyone cites when discussing their fears about death from going unvaccinated), you ALSO have to accept having your child injected with a whole bunch of stuff he or she does not need, and which may cause adverse effects. This is a very important concept. We, as concerned parents who love our children and want what’s best for them, are FORCED to give them MEDICATION (vaccines are medication – you can’t get them without a prescription, and they contain chemicals and things designed to alter the way your body functions) they DO NOT NEED, and which carries significant risk of side-effects. We do not FORCE adults to take medication even when they HAVE an illness, at least we didn’t, prior to COVID…
There are laws to protect adults from government-mandated medication. You cannot legally force a person with schizophrenia to take anti-psychotic medication, even when that person has already displayed violent aggression to others. You can’t legally force an adult cancer patient to take chemotherapy or radiation. If the government cannot force people to take medication when they HAVE an illness, how is it the government can force parents to consent for our infants and children to be injected with medications for illnesses they do not even have, and for which they have an extremely low risk (in many cases zero) of contracting?
Some will argue that nobody is “forcing” us to vaccinate. Thankfully, we do have some options, but we also give up a lot of our rights in the process. Many of us have to leave the workforce because our children are not allowed to attend daycare. Many of us lose our jobs because our children are so sick from vaccine-injury that we are FORCED to stay home full-time, whether that was our initial intent or not. Many of us are FORCED to become dependent on the government for financial assistance, especially if our marriages fail because the constant stress of caring for a sick child is overwhelming, financially, emotionally, and physically.
Many of us are lumped together in a big group and labeled “Anti-Vaxxers.” Some of us ARE Anti-Vaxxers. Some of us have been forced into being “Anti-Vaxxers” because we have no other choice. This is not a position we have chosen for ourselves and for many of us it is not an easy stance to take. We are simply doing our own research and weighing the costs-vs-benefits for our own children. At least that’s how it starts out. What happens in the process though, is we start to learn the truth about vaccines. We learn that they have not been studied for safety. We learn that they are implemented very quickly into the schedule without regard for their effects on “vulnerable populations.” As we research, we start to see patterns and we realize more and more how our children are not so rare, and how more children are being harmed everyday by mass vaccination. That’s when we become increasingly vocal. That’s when it becomes not just about protecting our children but about trying to protect your children, too. We realize that in many cases our concern for your children is not something you welcome. We realize that you wish we would just shut-up and go away. Many of us realize these things because we used to be you.
The reason we keep doing what we do is because we wish, beyond anything you can possibly comprehend, that someone would have done for us what we are trying to do for you.
You don’t have to agree with us. You don’t have to think we are right. You don’t have to be our friends.
We really do hope that you never know what it is like to be one of us. However, we also know that unless things change, our club is going to keep growing. If you become one of us, we will accept you unconditionally, and we will do everything we can to help you.
That’s just what we do.
Marcella.
I just don’t get how the medical community can celebrate the fact that they have been doing ABO-incompatible heart transplantation in infants for over 30 years due to the discovery that up to 14 months old the infant immune system is too immature to identify and reject a non-matching blood type and at the same time suggest that the same immature immune system should receive a boatload of vaccines.
It seems to be complete insanity that intelligent medical professionals can honestly not see the problem
If they're vaccinated why does it matter if an un vaxed kid is near them, they are supposed to be protected, by having the bloody jab, also un vaxed if theyre ill are off school, mostly, so, still the vaxed are safe. Biggest profitable con job ever ....Sick.