
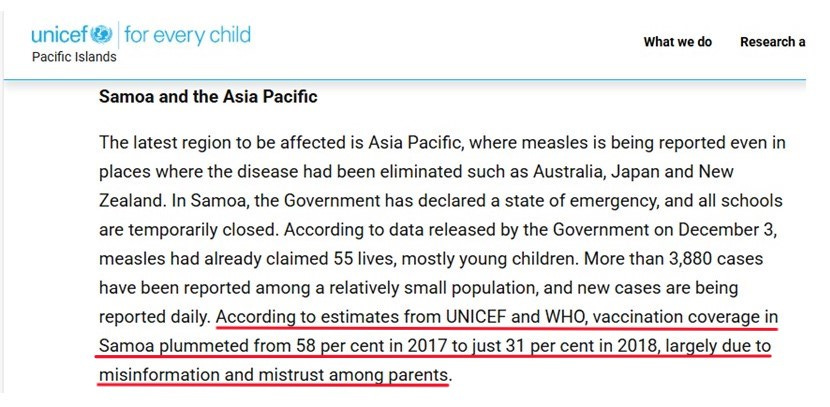
What really happened in Samoa in 2019? Is Robert F. Kennedy, Jr. really to blame for the deaths of 83 Samoan infants and children?

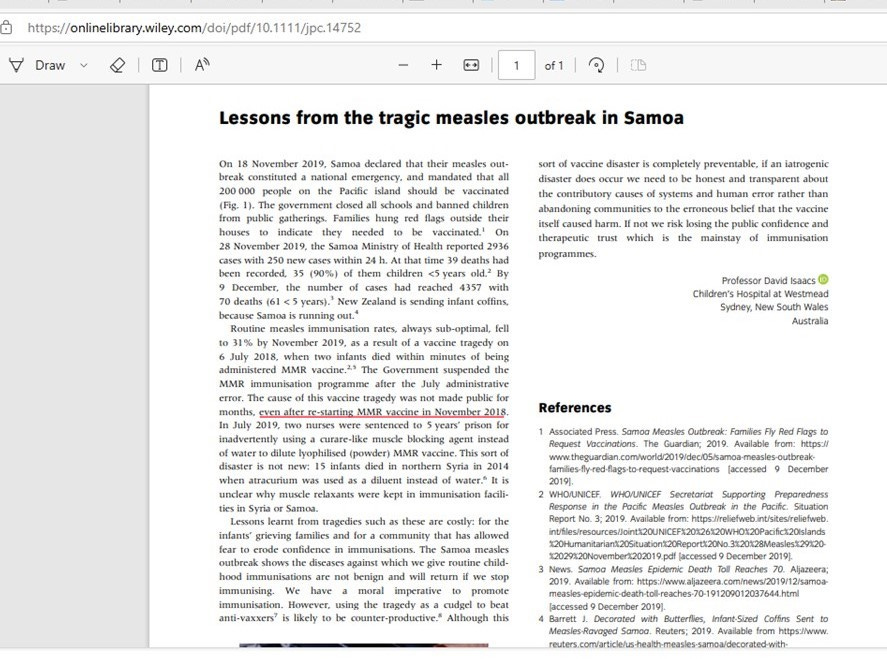
The 2019 measles outbreak in Samoa is a chapter in history that must not go unexamined. The story we hear from the media and from vaccine proponents like Paul Offit goes like this:
Once upon a time in a kingdom far away, all was happy and blissful until the anti-vaxxers invaded the peaceful island and used their cunning and manipulative methods to convince the island-folk that the white man’s medicine was bad. Because of the anti-vaxxers, the people of Samoa turned away from the life-saving needles and their magical contents, and as a result, the MMR vaccination rate dropped down to 31% coverage and this caused a HUGE OUTBREAK OF MEASLES, which ultimately ended up killing 83 people, mostly babies and young children. The heroes of the story are the Ministry of Health, the WHO, and UNICEF, whose valiant soldiers came to the rescue of the poor, defenseless islanders, with multiple doses of MMR vaccine for everyone – and especially for the babies and children. The knights in their white coats worked tirelessly, day in and day out, fanning out across the tiny island nation, seeking out and injecting all of the islanders who had been left defenseless by the wicked schemes of the anti-vaxxers, never ceasing nor pausing from their work until 95% of the islanders had received not one, but two doses of MMR vaccine, thereby reaching the pinnacle of protection – that elusive and very magical place called “herd immunity.” The end.
This fairytale is the official narrative on what happened in Samoa in 2019. The fairytale is now being used as a political tool, as you can see and hear in this recent PBS interview with Paul Offit:
And the way it works into Samoa is, they have a MMR vaccine in powdered form. It needs to be diluted in water. Two nurses made a mistake. Instead of diluting it in water, they diluted it in a muscle relaxant. Those children stopped breathing and died immediately.
Now, very quickly, within two weeks, it was realized what that mistake was. It was a nursing error. But, nonetheless, RFK Jr. seized on that. He flooded Facebook with information that measles vaccine is killing children in Samoa. He went to Samoa. He met with anti-vaccine activists. He met with senior officials in Samoa and kept the drumbeat alive that measles vaccine was killing children in Samoa.
As a consequence, vaccination rates fell from 70 percent to 30 percent. And between September and December of 2019, there was a massive measles epidemic. In this island nation of 200,000 people, there were 57,000 cases of measles and 83 deaths. Most of those deaths were in children less than four years of age.
And Robert F. Kennedy Jr. had everything to do with that. And that shows you how disinformation can kill.
Clearly, Offit is bringing Robert F. Kennedy, Jr. into the story because every fairytale needs a really good villain, and the fact that RFK, Jr. is on track to become the next head of Health and Human Services (HHS) makes him the perfect choice. He is handsome. Brilliant. Rich. And, according to Offit, very dangerous. However, as per the course, Offit does not have his facts right. As is his usual modus operandi, he confuses fact with fiction and when spewing figures, he doesn’t miss a chance to greatly exaggerate the magnitude of the measles outbreak, multiplying the actual number by a factor of ten. No, Paul. There were not 57,000 cases of measles in Samoa in 2019. There were 5,700 cases of something – and as the truth will reveal – some of them may have been actual measles. It’s hard to say just how many cases were actual, wild-type measles (aka “classical measles”) and how many were modified measles (aka “atypical measles”). That’s because pretty quickly after the “outbreak” began to blow up in terms of numbers, the Ministry of Health and the WHO made the decision to stop laboratory testing. But alas. I’m getting ahead of myself. Let’s start at the beginning…
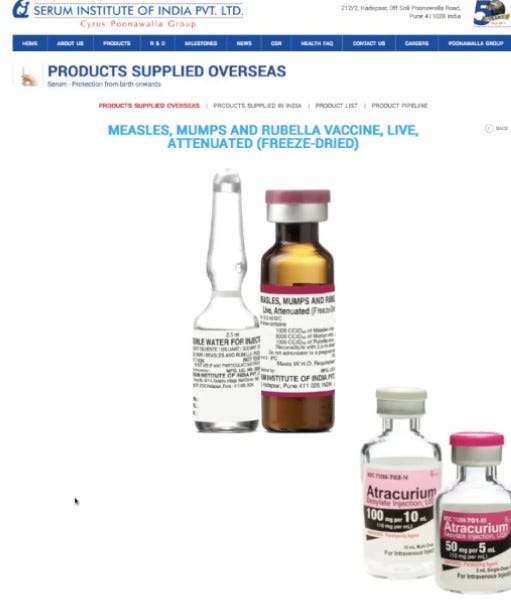
July 6, 2018: Two babies die within minutes of receiving an MMR vaccine. These tragic deaths happened after the babies were injected at the same clinic, from the same batch, and from the same vial. The public was left in the dark for weeks during the resulting investigation, which centered on two nurses. One was a senior nurse with many years of experience. The other was a less experienced nurse who was under the supervision of the senior nurse. The story goes: The senior nurse (who has been administering vaccines for a long time) mistakenly used a vial of expired anesthetic (Atracurium - which is only used in surgeries, and which somehow made its way into the refrigerator at the vaccine clinic) instead of water to reconstitute the powdered MMR vaccine. The junior nurse did the injecting. After the death of the first baby, the story goes, there were expressed concerns about continuing to use the MMR vaccine that had been mixed up a few hours prior, and which had been injected into the now deceased baby, but the senior nurse refused to mix a new vial, and, going against colleagues’ advice, she instructed the junior nurse under her supervision to use the same vial, injecting a second child who also died within minutes.
According to the local news reports, the senior nurse then concealed evidence, taking the vial home with her and keeping it hidden from the authorities. That part certainly seems to bring some truth to the story. However, it’s kind of confusing to consider how a senior nurse who’s been a seasoned vaccinator for years, could confuse the bottle of water and the bottle of Atracurium. They’re quite different in their appearance. And… what was Atracurium doing in the vaccine fridge?? It’s one of those things that make you go “Hmmmm…..”
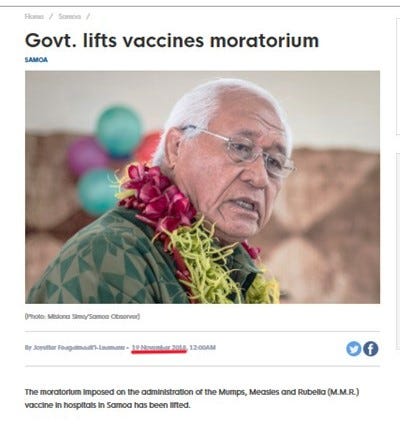
Anyway… What the public knew about the situation, for at least a few weeks, is that two babies died within minutes of the MMR vaccine. Understandably, a lot of parents were not eager to line up with their babies to see if their child might be next. And… contrary to Paul Offit’s fantasy that the vaccine coverage rate dropped because of RFK, Jr., it was the Samoan Ministry of Health’s issuance of a moratorium on the entire MMR vaccination program that caused a cessation in injections and a resultant drop in “vaccine protection from measles.”
Was it so preposterous to believe the MMR vaccine itself may have been the cause of the babies’ deaths?
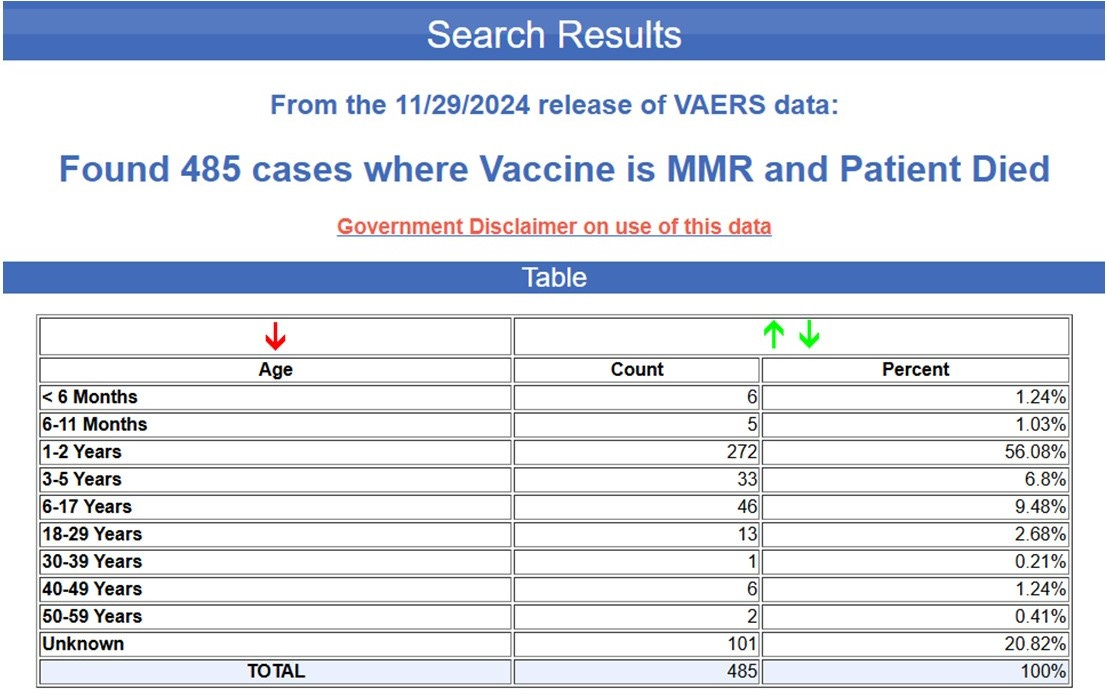
I did a quick search of the VAERS data for death from MMR vaccine. Here are the numbers:
As of November 29, 2024, there have been 485 deaths from MMR vaccine reported to VAERS.
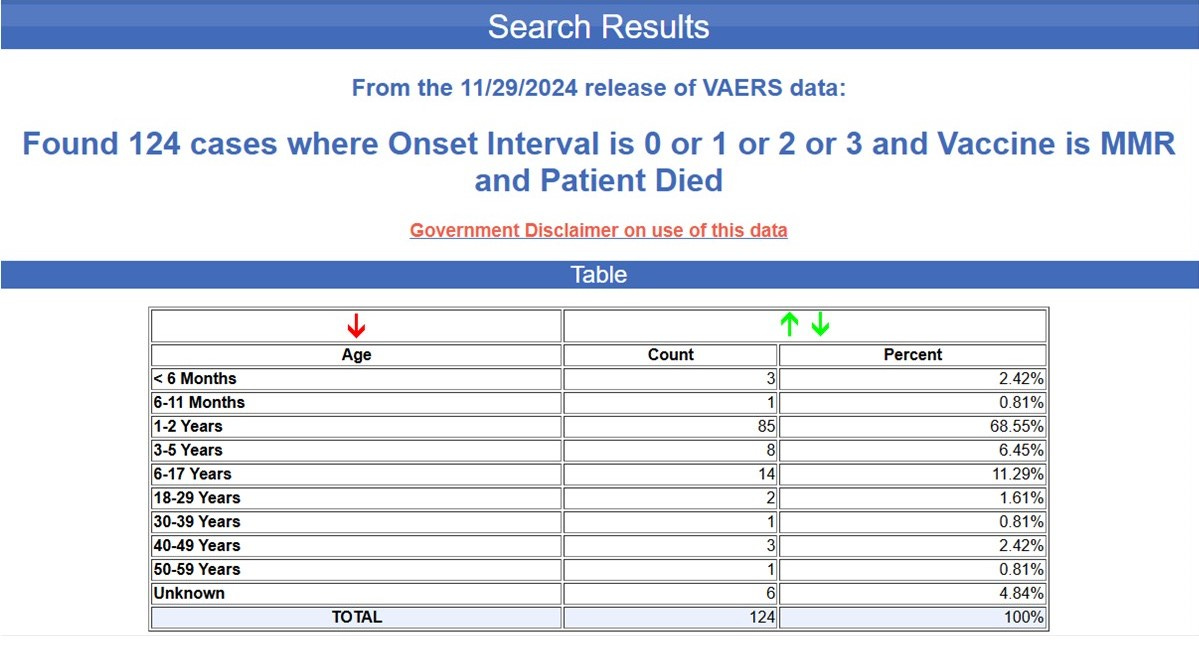
Of the 485 deaths from MMR reported to VAERS, 124 deaths occurred within the first three days after vaccination.
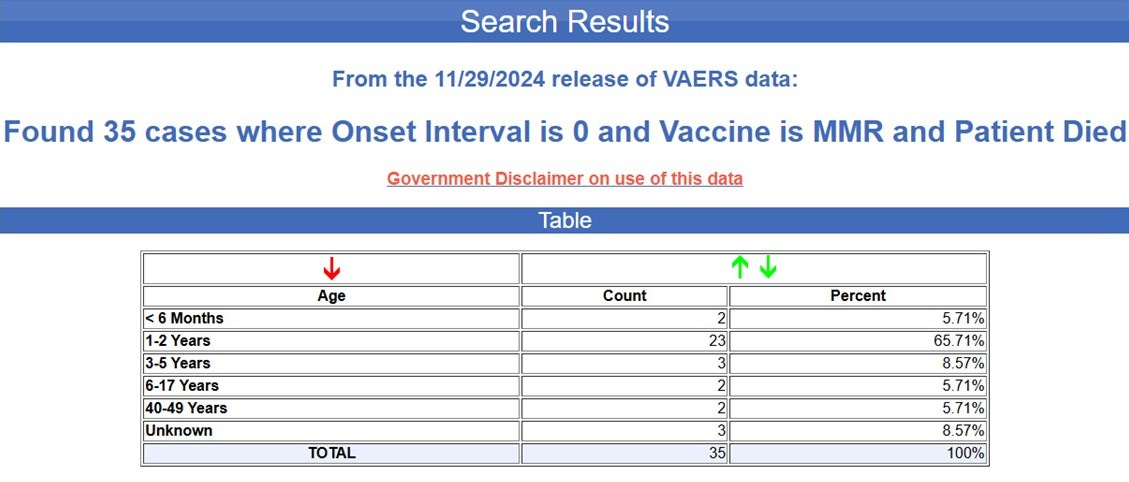
Of the 485 deaths from MMR vaccination reported to VAERS, 35 deaths occurred on the day of vaccination. Within minutes or hours. For anyone who doesn’t know, the numbers reported to VAERS are a VAST underestimate of the actual injuries and deaths caused by vaccination. A study that was commissioned by the United States Department of Health and Human Services (the umbrella organization that includes the CDC) to study the VAERS database found that less than 1% of even the most serious adverse events from vaccines are reported to VAERS. The CDC stopped communicating with the researchers and halted the study after learning the findings. You can read the report here.
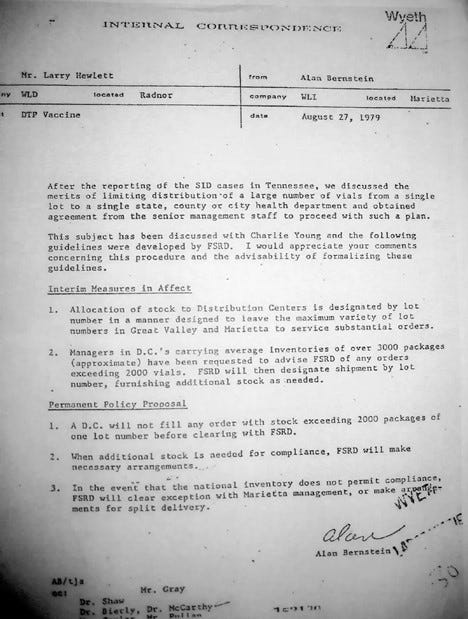
I will be the first to admit that it seems a bit of a “conspiracy theory” to question the official narrative about what happened to the two babies who died in Samoa on July 6, 2018, within minutes of receiving an MMR vaccine from the same vial/batch. Color me jaded, but it’s less difficult to imagine when you understand that similar cover-ups have happened before. Have you heard about the Tennessee SIDS Cluster? If you don’t know about it, now is a good time to read… Here are a couple of good articles that explain what happened and how the vaccine manufacturer (Wyeth, in this case) conspired to hide the fact that its DPT shot was killing babies. Click here and here. As a teaser, here is the internal memo, in which the makers of the DPT make the decision to split up their vaccine lots after realizing that by sending too many vials of a single lot to any one geographic location, it made it way too obvious when multiple deaths occur within 24 hours of receipt of that vaccine. Instead of working to improve the safety of their vaccine, they decided to actively conceal the deaths - those that had already happened and those they knew would continue to happen after the Tennessee SIDS Cluster.
When one understands the lengths to which the vaccine industry will go to conceal the dangers of their products, questioning the official narrative in the Samoan MMR incident sounds less and less like a conspiracy theory and more and more like a conspiracy reality. I do struggle with the report that the senior nurse concealed evidence and took the Atracurium vial home to hide it. However, I have also read enough and watched enough television in my 65 years to know that evidence gets planted, and given the history of the industry’s behavior, it seems to me that throwing two Samoan nurses in front of the bus is not out of line with the expected response. I learned a long time ago that the best predictor of future behavior is past behavior. Vaccine makers (and the CDC and all who denied the validity of the vaccine-induced deaths in Tennessee) had no qualms at all about moving forward with the DPT shot when they knew it was killing innocent babies. The lives of two nurses seem a small sacrifice in comparison.
Paul Offit – and the cadre of MMR vaccine promoters and measles fear-mongerers keep repeating the inaccurate statement (lie) that at the time of the measles outbreak in October and November of 2019, the MMR vaccination rate among 12-month-old Samoan children was 31%. Where did this number come from, and how accurate is that statement?
The initial government moratorium on MMR vaccination in Samoa began in July 2018 and was to continue for ten months. However, during that time, the investigation into the two nurses was ongoing, and once they were arrested and charged, the government restarted the vaccine program. Not once, but twice. The first time the MOH restarted MMR vaccination was in November of 2018.
(source)
(source)
The second announcement was made on April 1, 2019, as you can see in this Facebook video from the Government of Samoa, in which the Director of the Ministry of Health announces that “The MMR is 100% safe” and a new, more aggressive mass vaccination campaign employing the Catch-up Schedule will begin on April 15, 2019.
The mass vaccination “catch-up” program was so aggressive that by the end of June 2019 – three and a half months before the start of the measles outbreak, the Samoan Ministry of Health reported an 80% MMR coverage rate among 12-month-old Samoan children.
This is the cover page of the Ministry of Health’s Financial report for 2018-2019.
This is the signature page of the same document, showing that the information contained within covered the period of time through the end of June 2019.
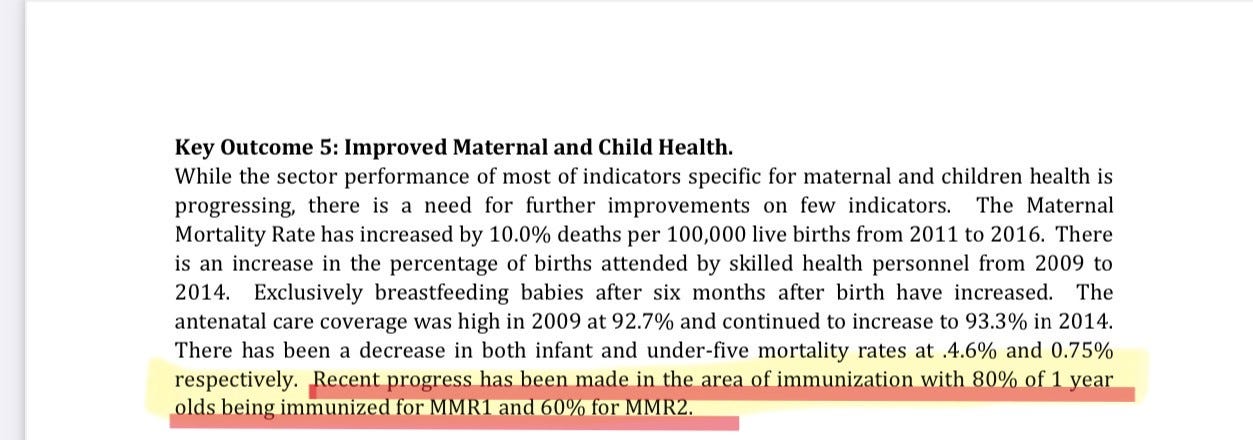
From page 9 – the Samoan Ministry of Health reported that “RECENT PROGRESS” – through mass vaccination, resulted in an 80% coverage rate for the FIRST dose of MMR vaccine and a 60% coverage for the SECOND dose in 1 year old Samoan Children. Three and a half months before the start of the “measles outbreak.” (source)
Let’s go back to fact-checking Paul Offit for a moment.
In the interview with PBS News, Dr. Offit made the following statement about Robert F. Kennedy, Jr.’s alleged role in the Samoan measles outbreak:
Now, very quickly, within two weeks, it was realized what that mistake was. It was a nursing error. But, nonetheless, RFK Jr. seized on that. He flooded Facebook with information that measles vaccine is killing children in Samoa. He went to Samoa. He met with anti-vaccine activists. He met with senior officials in Samoa and kept the drumbeat alive that measles vaccine was killing children in Samoa.
As a consequence, vaccination rates fell from 70 percent to 30 percent.
Facts matter, Paul. So do timelines. As this NBC news article reports, RKF, Jr. did visit Samoa and met with MOH officials there, but his visit took place in June of 2019.
The rate of MMR vaccination in Samoa fell, beginning in July of 2018, as a result of the Samoan government’s moratorium on MMR vaccination, after the death of two infants. As the above documentation from the Samoan Ministry of Health clearly shows, the two MMR vaccination campaigns conducted in November 2018 and April 2019 resulted in an 80% MMR rate for the first dose and a 60% MMR vaccination rate for the second dose, and this was reported in the MOH’s public record, documenting progress through June 30, 2019. So, Offit is just plain wrong, and his accusations are completely FALSE.
What really matters for the purpose of the rest of this article is that as a result of two mass vaccination campaigns in November 2018 and April 2019, and a third mass vaccination campaign in November of 2019, tens of thousands of Samoans, including infants and children received not ONE but TWO doses of MMR vaccine just four weeks apart. A very pertinent question to ask is,
“Did the mass vaccination campaigns contribute to the outbreak that sickened thousands and killed dozens of people - most of them children?”
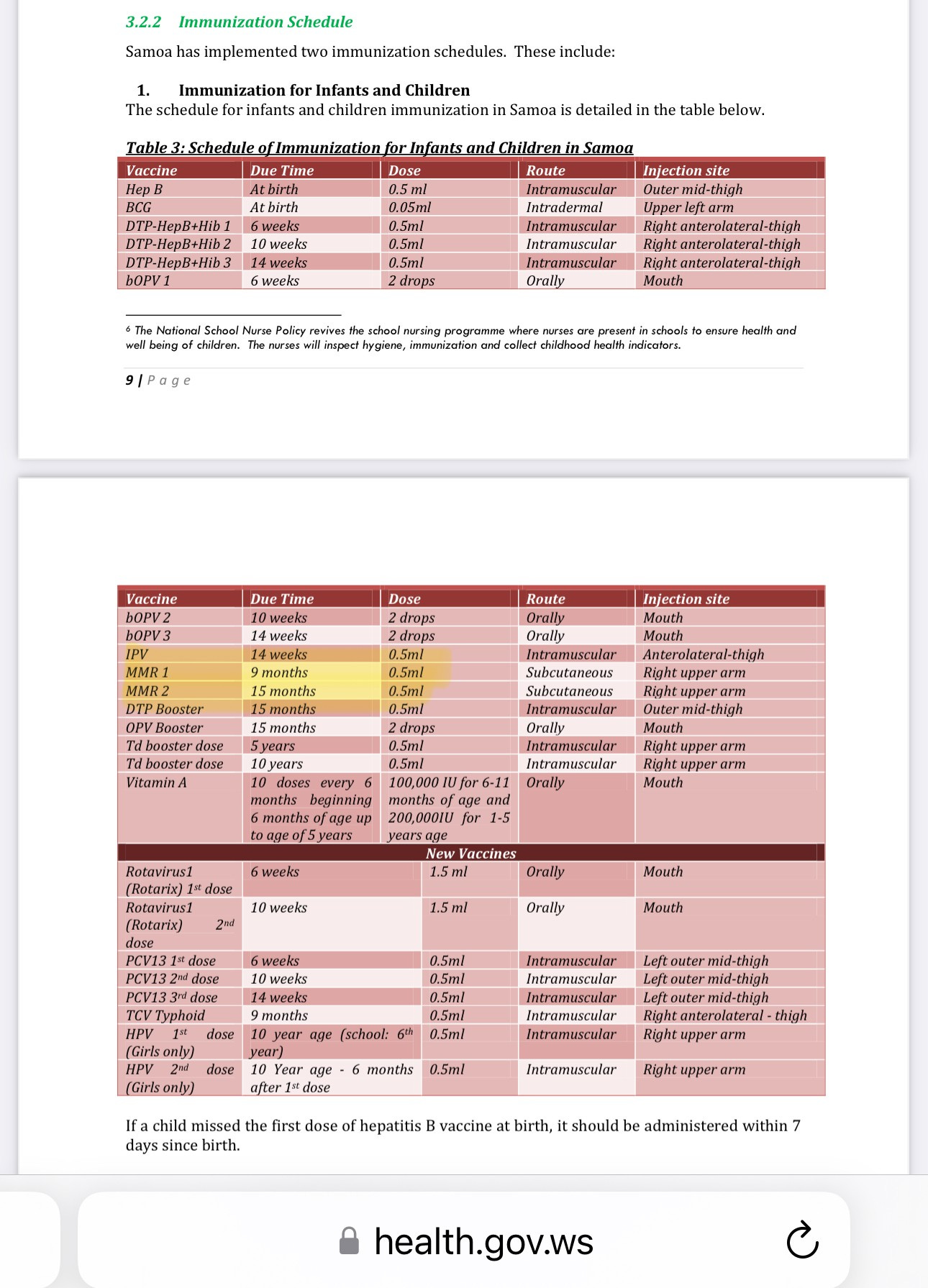
That’s a whole lot of babies and young children who were vaccinated in a very short period of time, with a live attenuated measles virus. For those who are not familiar, in developing nations, the vaccine schedule is different from the schedule used in first world countries like the United States and the U.K., where our children receive the first MMR at 15-18 months and the second MMR at 4-6 years of age. In developing nations, infants receive the first MMR (aka MCV – measles containing vaccine) at 9 months of age. The second MMR is given at 15 months.
Here is the Samoan vaccination schedule:
(source)
When using the “Catch-Up Schedule,” which is followed during mass vaccination campaigns designed to get to “herd immunity,” two MMR vaccines are given with the first one at 12 months (or later, for those who missed it “on time” at 9 months) and the second MMR vaccine given four weeks later.
This is the Samoan Catch-up schedule:
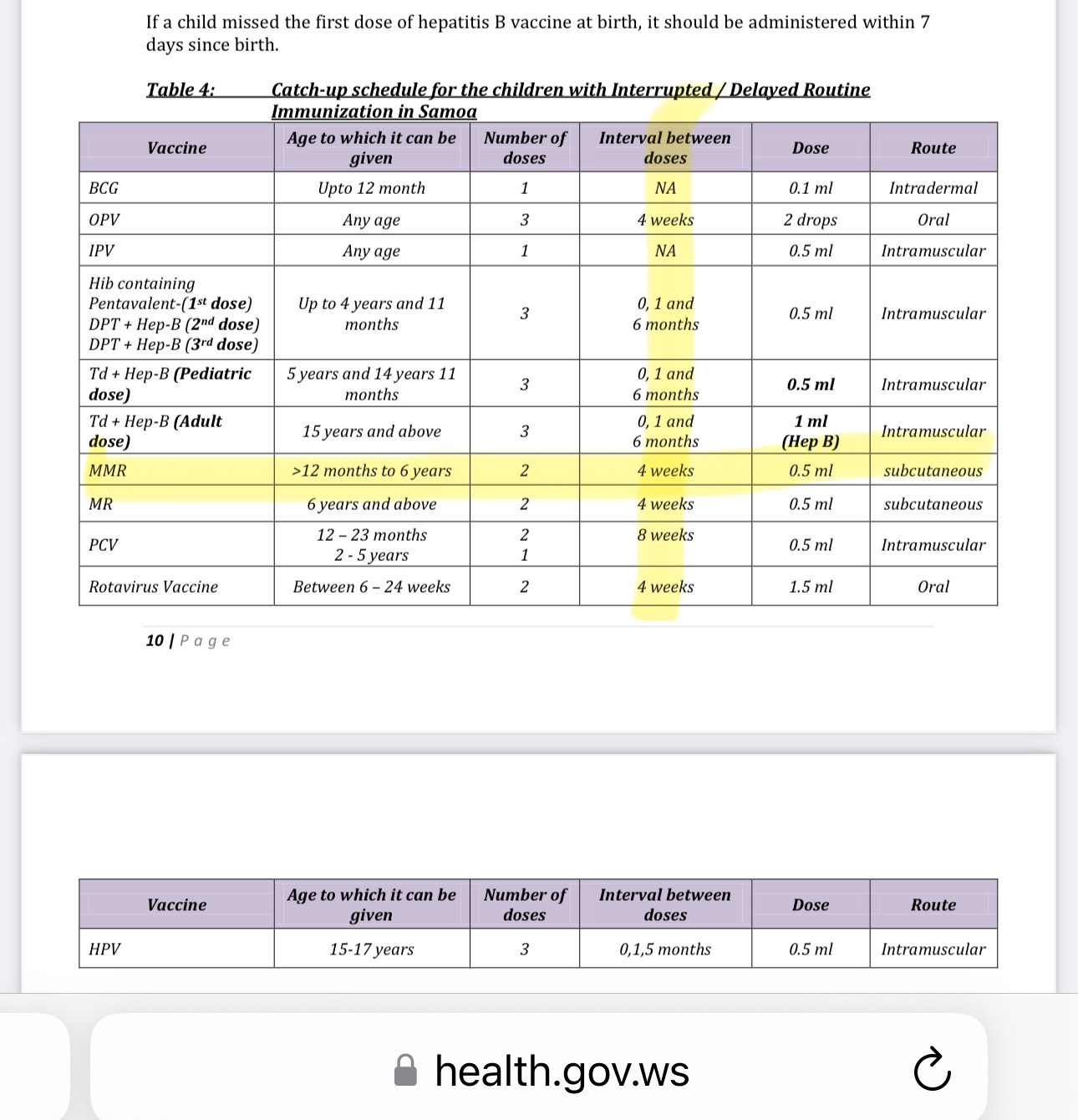
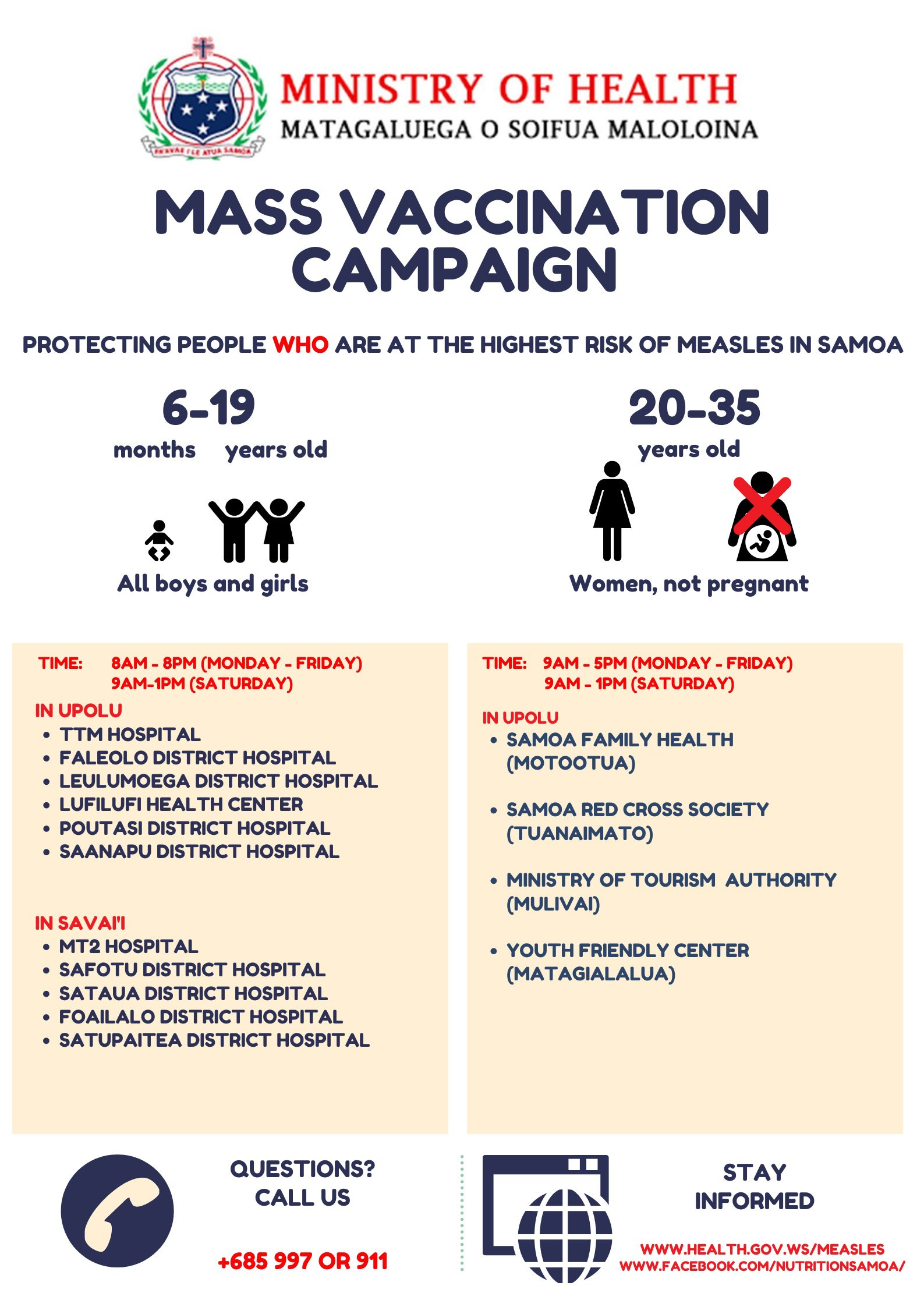
As aggressive as this schedule is, the situation was even more concerning in Samoa in 2019, when the government mandated MMR vaccination (two shots 4 weeks apart) for everyone six months of age and up.
Recap: What most people have heard by now is that the measles outbreak that occurred in Samoa in October through December of 2019 happened because when the outbreak began, the vaccination rate in one-year-olds had fallen to 31 percent coverage. What most people have heard is that the fall in vaccination coverage was due to anti-vaxxers, misinformation, and Bobby Kennedy. By now you have seen that according to the Samoan Ministry of Health’s official document, the actual rate of MMR coverage for one year-old Samoan children was 80 percent for the first dose and 60 percent for the second dose, and this was accomplished by June 30, 2019. But the aggressive vaccination campaigns did not stop at the end of June. They continued in the months leading up to and throughout the “measles outbreak” in October through December, greatly increasing the number of very young children who received two live virus MMR vaccines four weeks apart in the weeks and months leading up to, and during “the outbreak.”
Where did the “31% vaccination rate” number come from?
The narrative for the 31 percent rate is strong and has been repeated so many times it has become “true.” Where did that number come from? It appears to have come from UNICEF, in this report published December 8, 2019.
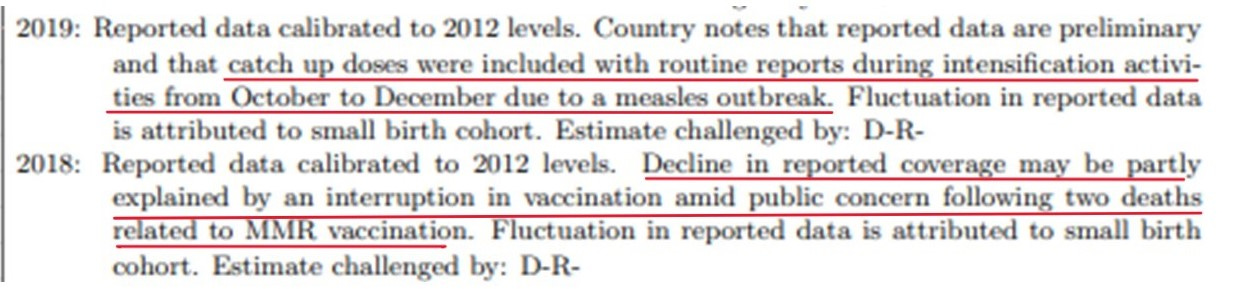
And here is another document. This one is titled, “WHO and UNICEF estimates of national immunization coverage” and was published by UNICEF on July 8, 2021.
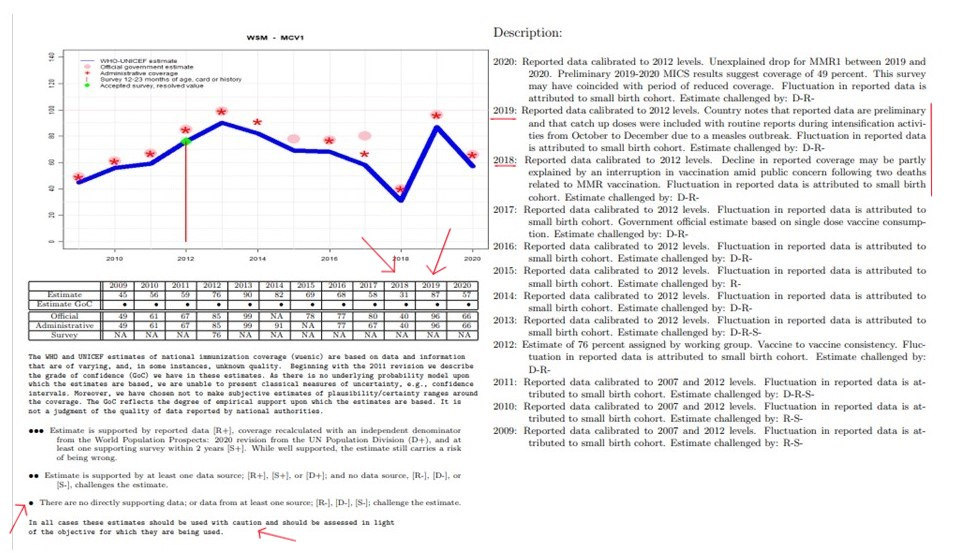
That’s some really tiny stuff. Here are the highlights:
The rate of MCV (measles containing vaccine) coverage in Samoa has never been very high and certainly was never anywhere near the magical 95% coverage we are all told has to happen in order to prevent outbreaks of disease and death.
In the four years leading up to 2019, the rate of MCV coverage was never above 70%, and yet, there were no measles outbreaks reported. That only happened AFTER the government of Samoa, UNICEF, and the WHO enacted their aggressive mass vaccination campaigns beginning in the spring and continuing through December of 2019.
Here are a couple of details from the document above, so you can see them better:
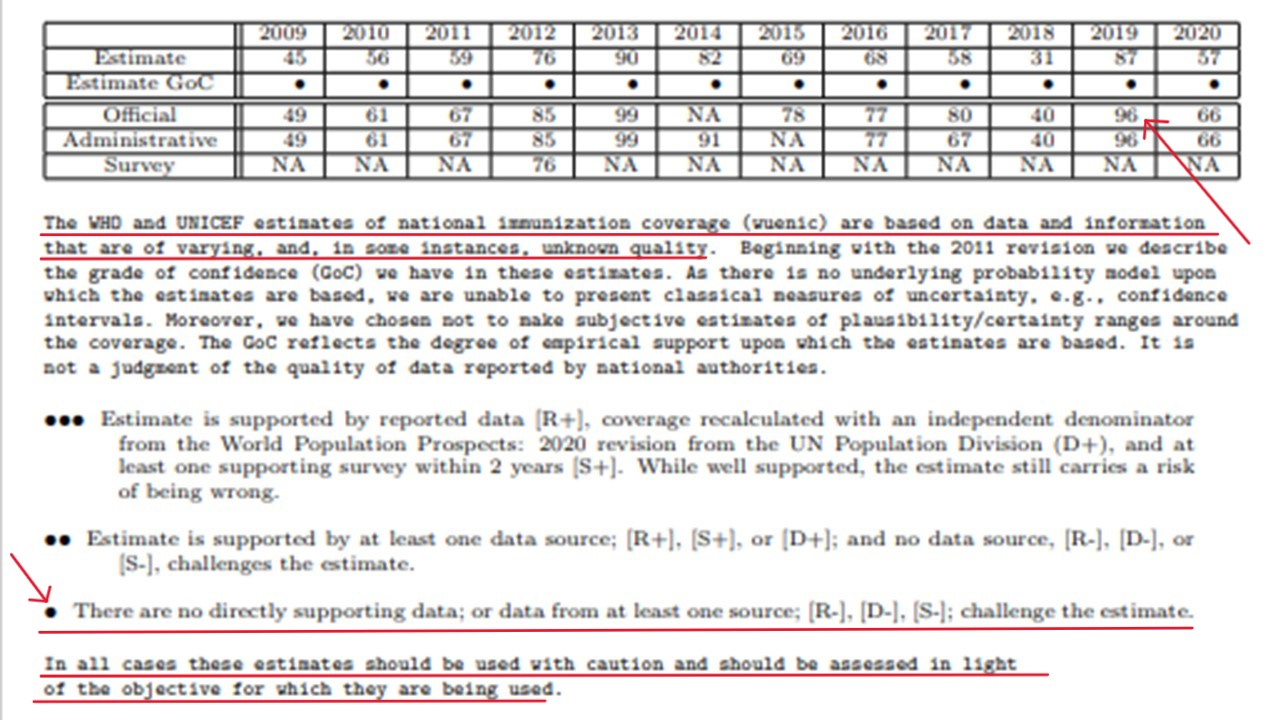
The WHO and UNICEF estimates of national immunization coverage (wuenic) are based on data and information that are of varying, and, in some instances, unknown quality.
There are no directly supporting data; or data from at least one source…
In all cases these estimates should be used with caution and should be assessed in light of the objective for which they are being used. (emphasis mine… just what was the objective for using the very sketchy 31% rate?)
I am reminded of a meme I made several years ago…
The real trouble for the people of Samoa began to heat up after the first potential measles cases were identified and samples sent for analysis on September 30th and October 2nd, with UNICEF and WHO descending on the island country, with door-to-door campaigns and mandatory vaccines for everyone. This aggressive mass vaccination campaign took place from October to December and coincided with the explosion of new measles cases, ultimately ending with the deaths of dozens of infants and children.
If we are to believe anything from the UNICEF and WHO report, the most likely believable result is that by the end of 2019, according to the “official” and “administrative” information, 96% of Samoan infants and children over the age of 6 months were vaccinated with the live MMR vaccine. Because the earlier estimates for years 2015-2018 indicated low coverage (below 70% in each year), we can safely assume there were considerable numbers of children between the ages of 1 and 4 years who were also targeted for mandated vaccination with two doses of MMR four weeks apart, as per the catch-up schedule.
This November 25, 2019 tweet from the Samoan Government gives us an idea just how massive their mass vaccination campaign was.
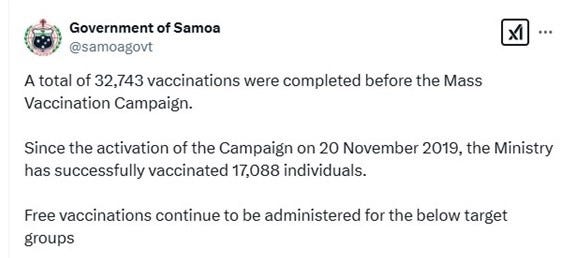
So now we know that by November 25, 2019, there had been a total of nearly 50,000 MMR vaccines administered in a very short time frame in response to the measles outbreak. The population of Samoa is roughly 200,000 people, so 50,000 vaccines is a very big deal in that group.
According to this tweet from the Samoan Government, 90% of the Samoan population had been vaccinated as of December 8, 2019.
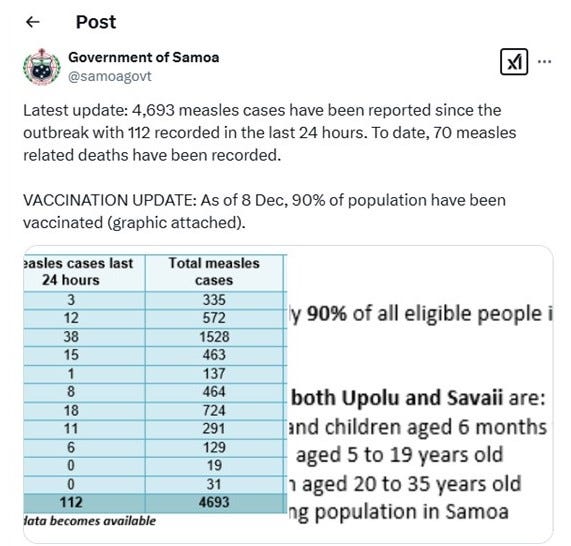
Here is the graphic from the Samoan Government, from December 8, 2019:
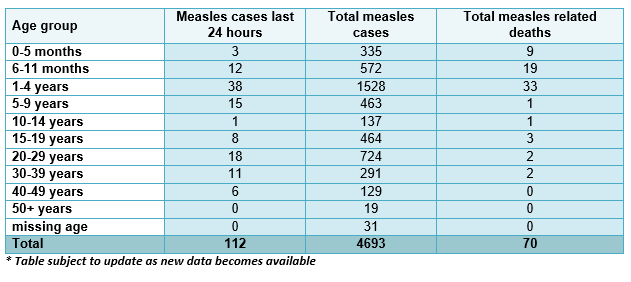
I find it interesting and concerning that the vast number of cases of measles and measles related deaths are in the age groups that were most heavily targeted for vaccination.
What does the timeline of events look like?
Let’s look at the timeline of events, constructed by Professor Ian McCay, Ph.D. (Virology).
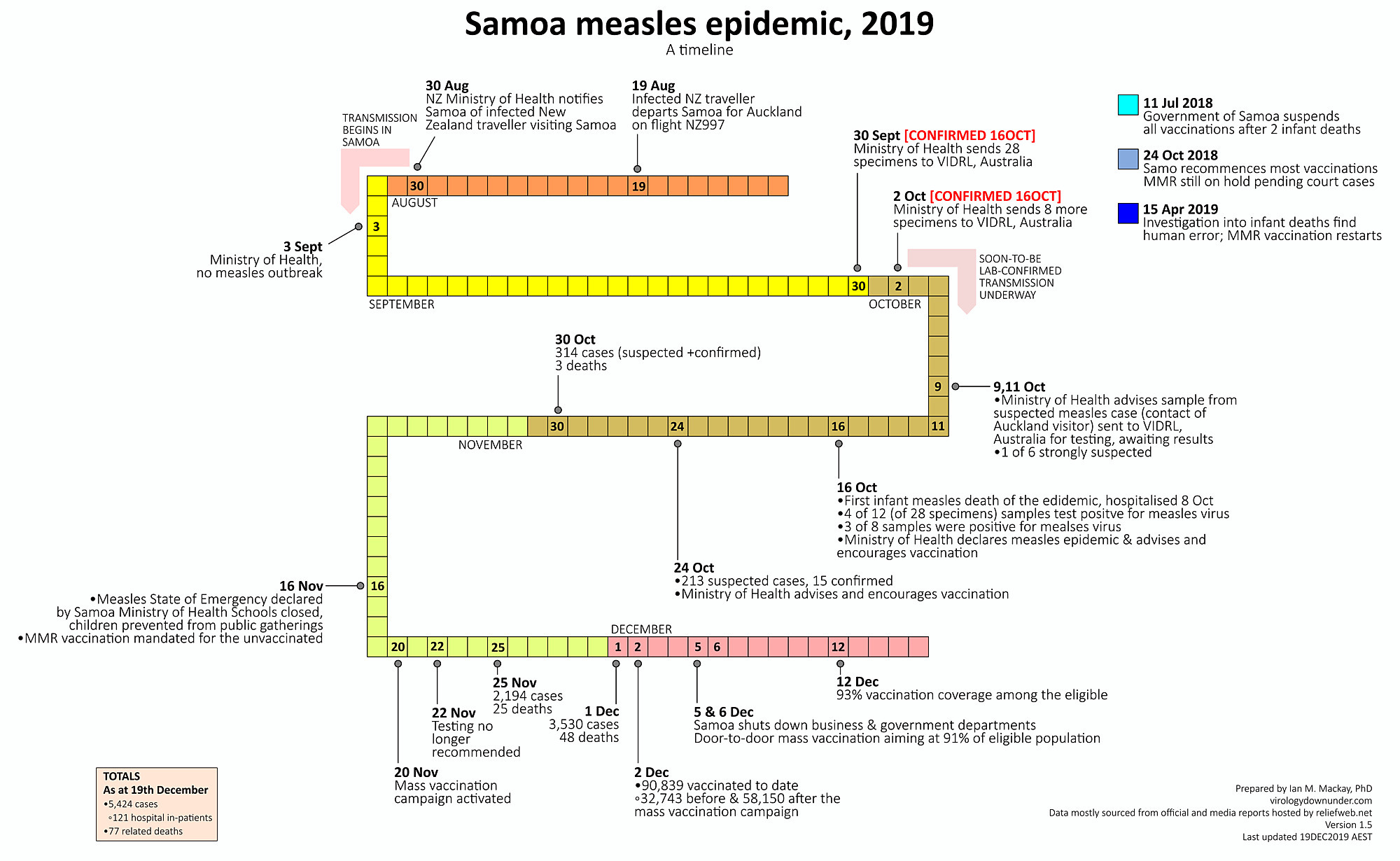
Timeline:
August 19, 2019 - a traveler from New Zealand who was infected with measles arrives in Samoa. The government of Samoa is informed on August 30th.
September 3rd - the government of Samoa declares no measles outbreak as a result of the infected traveler. Note that the incubation period (time from exposure to onset of symptoms) for measles is typically 11-12 days, according to the CDC. That means that if the New Zealand traveler had been responsible for the measles outbreak in Samoa, cases of measles should have been evident by August 31st. According to the Samoan government, there were no cases of measles as of September 3rd. According to the timeline, all was quiet until September 30th.
September 30-October 2 - The Samoan government sends 36 samples from suspected measles cases for laboratory analysis.
October 1 - UNICEF begins delivering vaccines and the ongoing mass vaccination programs increase in scope.
October 16 - Seven of the 36 (19.4%) samples submitted for laboratory analysis were confirmed measles. Government declares measles epidemic and advises vaccination.
October 24 - 213 suspected measles cases, with 15 (7%) confirmed by lab analysis.
October 30 - 314 “suspected + confirmed” cases. Three deaths.
November 16 - State of emergency declared, schools closed, children prevented from public gatherings, MMR vaccination mandated for the unvaccinated.
November 20 - Mass vaccination (#3) campaign activated.
November 22 - Laboratory testing no longer recommended.
November 25 - 2,194 (unconfirmed) cases, 25 deaths.
December 1 - 3,530 (unconfirmed) cases, 48 deaths.
December 2 - 90,839 vaccinated to date; 32,743 before & 58,150 after mass vaccination campaign initiated on November 20th.
December 5 & 6 - Businesses shut down, door-to-door mass vaccination aimed at 91% of population
December 12 - 93% vaccination coverage among the eligible.
So now we know that among the people who got sick in October and early November in Samoa, a very low percentage of those cases (7-19%) actually tested positive as being measles. We also know that the cases and deaths increased exponentially after UNICEF began their vaccination campaign on October 1st, and the cases and deaths continued to increase at an even higher rate following the declared mass vaccination campaign on November 20th. And two days later, the Samoan government issued an order to stop testing.
Why did the Samoan government stop testing?
Why didn’t they want to know just exactly how many of the “suspected measles cases” and “suspected measles-related deaths” were actually due to measles? Was it because if they continued testing after the mass vaccination campaigns, they would have to admit that many of those “suspected” cases were actually vaccine-associated measles and vaccine-associated deaths?
WHOA, NOW!!! That’s a BIG accusation without any proof!
Read on…
What was the health status of the Samoan population?
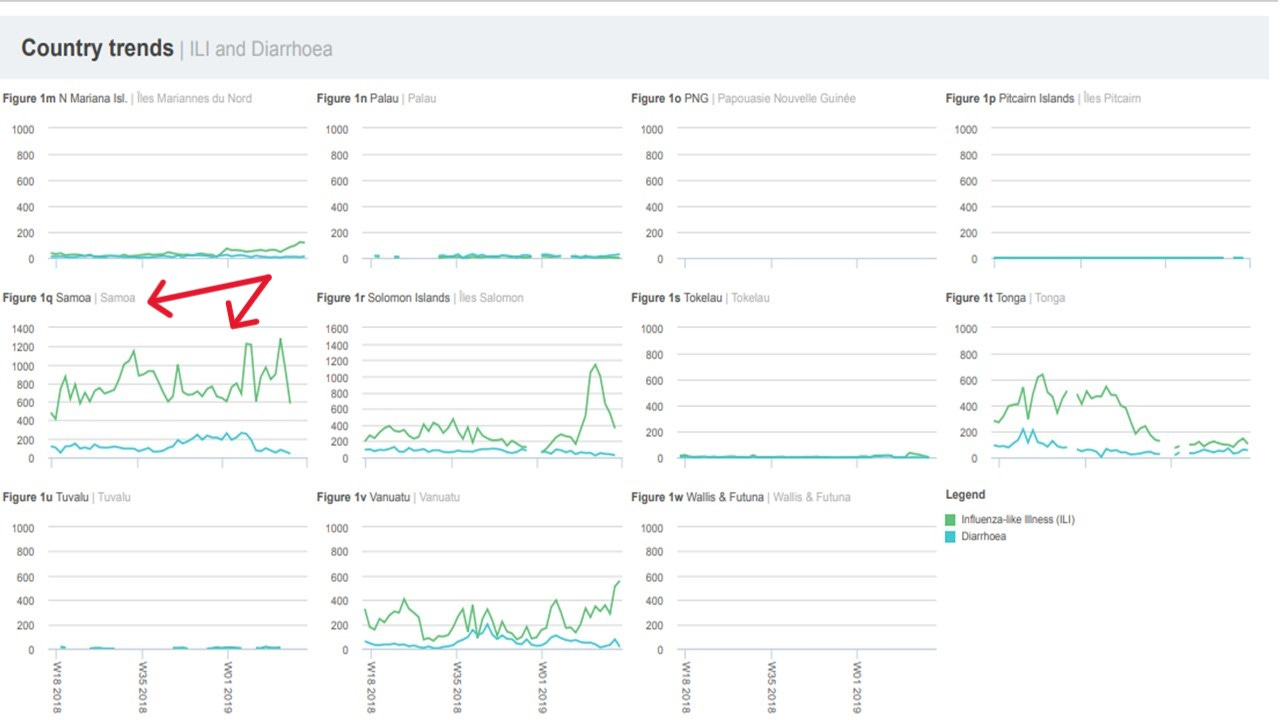
In order to assess the likelihood that mass vaccination may have negatively affected the people of Samoa, and especially the infants and children, we need to look at the health status of the Samoan population, prior to and during the measles outbreak. Here is where you can find the World Health Organization’s data on the overall health status of the country, in weekly reports. The following set of graphs shows the incidence of influenza-like illness (ILI) and diarrhea in the Samoan population compared to neighboring Pacific Island nations in April of 2019, at the time when the first mass MMR vaccination campaign began. As these graphs show, the incidence of influenza-like-illness and diarrhea was considerably higher in Samoa than in neighboring nations. This is a robust indication that the overall health of the Samoan people was certainly less than optimal and may have put their children at increased risk of serious adverse reactions to vaccination with MMR.
Additional information about the health of the Samoan population can be obtained by reviewing the Demographic Health Survey (DHS) conducted by the Samoan Government. This survey was conducted in 2019-2020 and published in May of 2021.
Here are a few of the key findings:
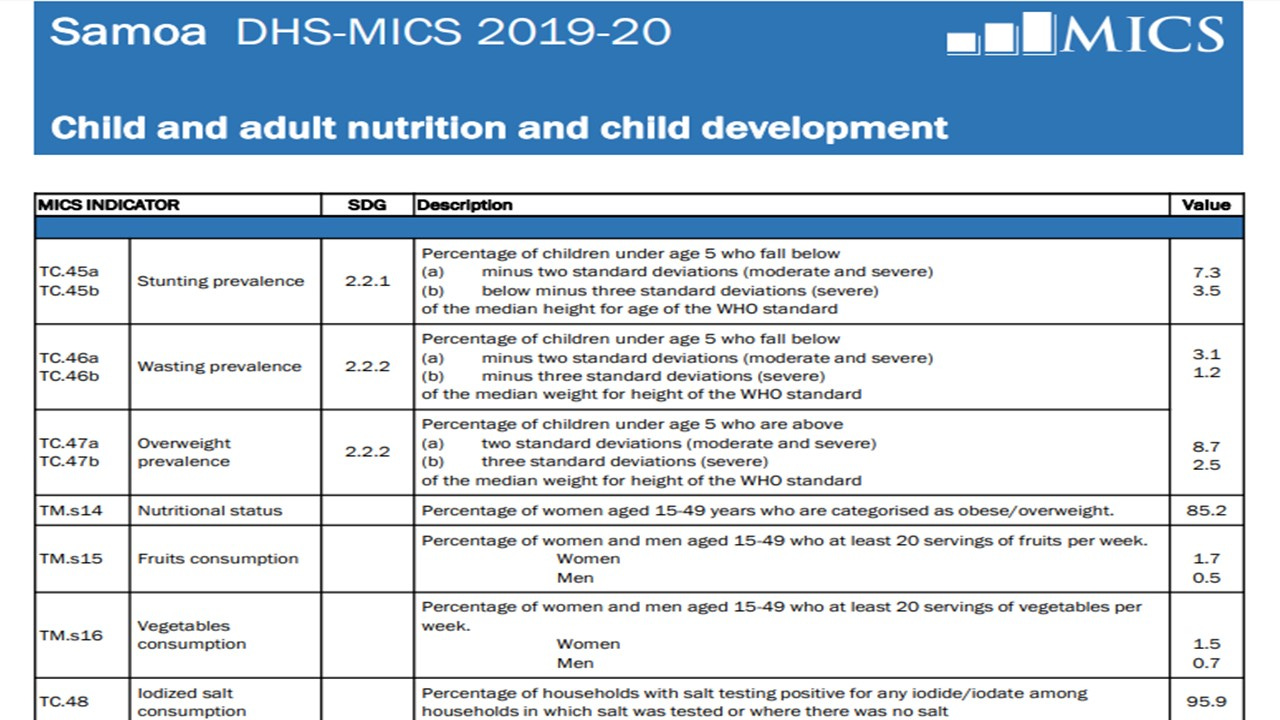
Among children under the age of five years, 15.1% met the criteria for Stunting or Wasting, indicating severe acute malnutrition (SAM) status.
Among children under the age of five years, 11.2% were significantly overweight or obese.
Among women aged 15-49 years, 85.2% were obese/overweight.
The percentage of Samoan adults who consumed the minimum recommended number of servings of fruits and vegetables per week was between 0.5% and 1.7%.
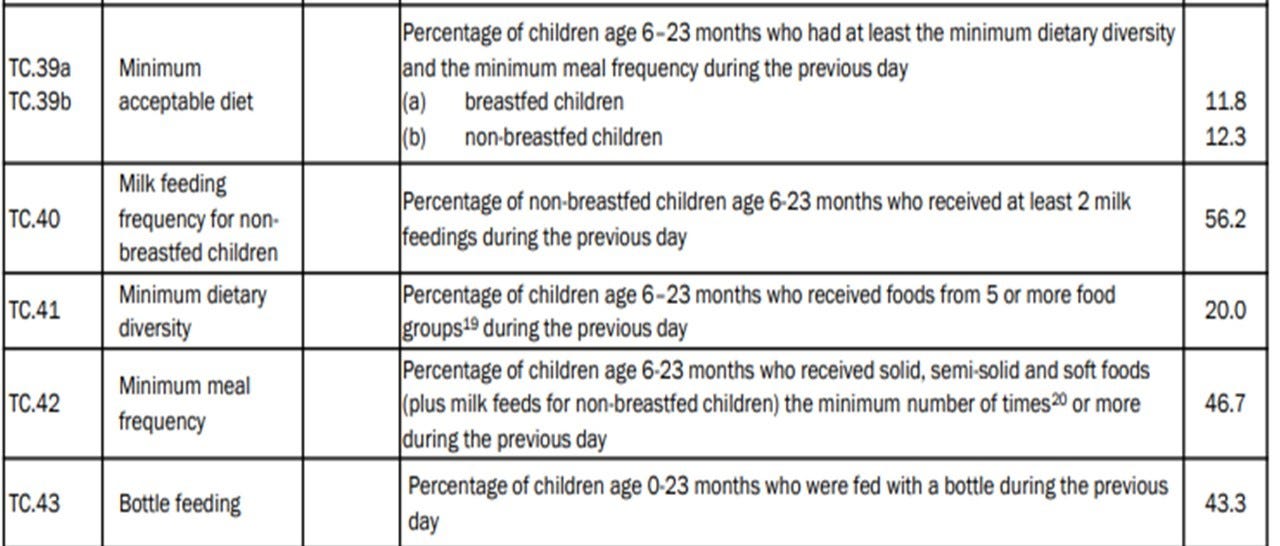
Among children aged 6-23 months, only 20% (1 in 5) met the criteria for minimum dietary diversity.
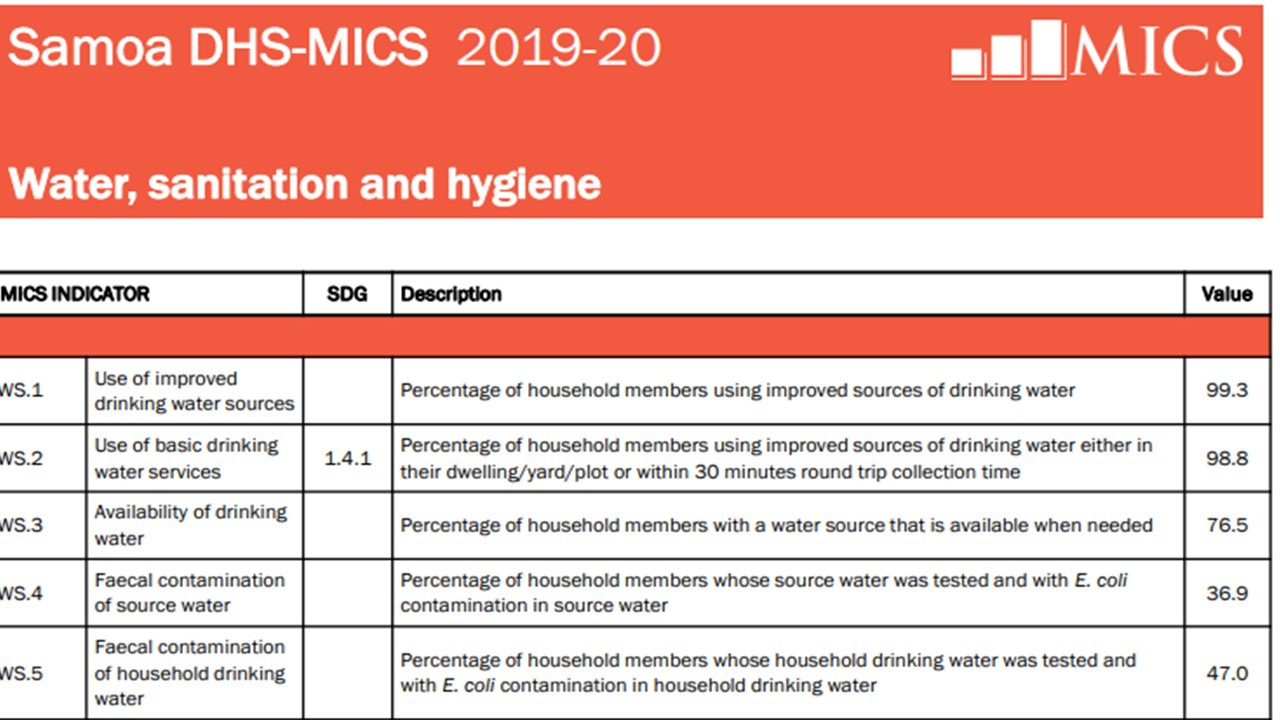
47% of households had drinking water with fecal contamination from sewage
The fact that nearly half of all households in Samoa had drinking water that was contaminated with fecal matter (from sewage) is highly significant and was most likely a factor involved in the growth of the outbreak. If fecal matter was in the drinking water, it’s highly likely that urine was also in the drinking water. And THAT is very problematic when it comes to the spread of vaccine-strain measles, as the following article from the peer-reviewed medical literature indicates.
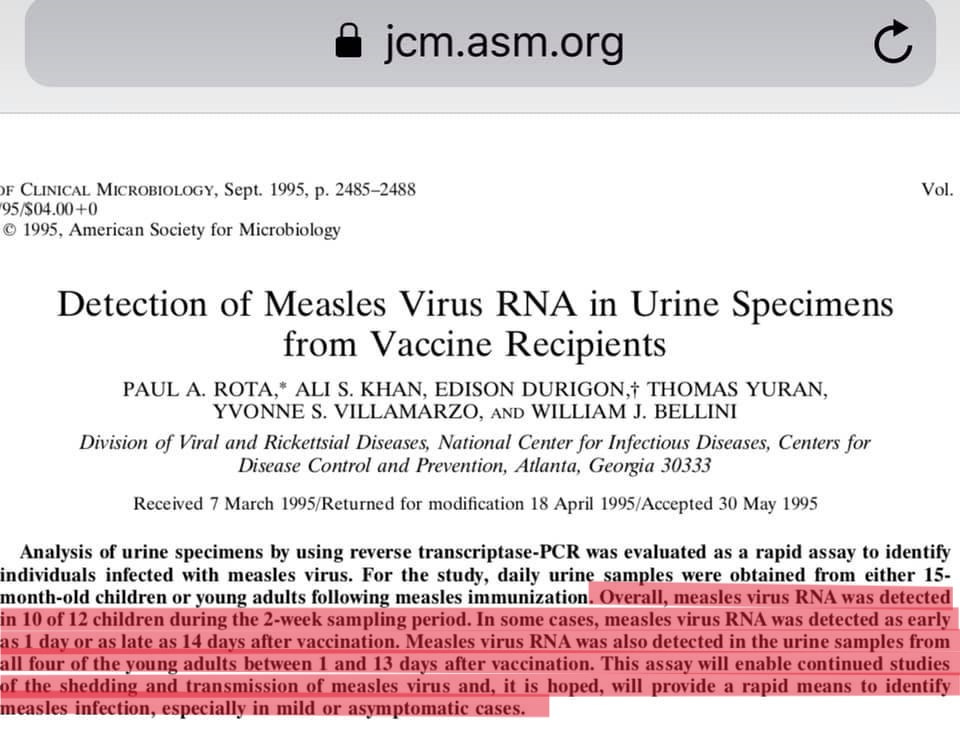
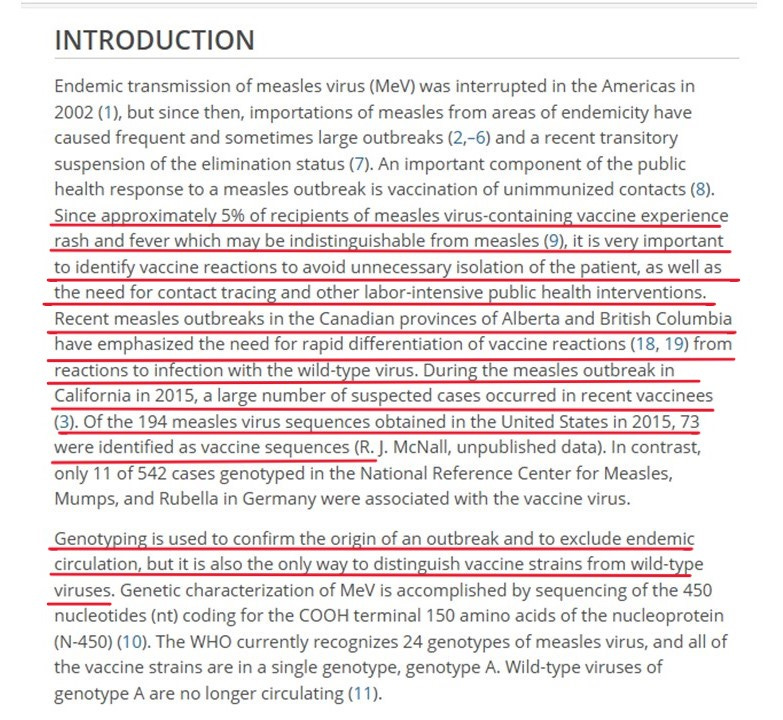
Vaccine strain measles sheds in the urine of vaccine recipients for at least two weeks after vaccination. As the authors note, this is important information for understanding the “shedding and transmission of (vaccine-strain) measles virus (source).” With more than 90,000 MMR (live virus) vaccines administered over a period of a few months in a nation of 200,000 people, where nearly 50% of the drinking water is contaminated with fecal matter (and urine), one can easily understand why this would be problematic. The fact that the drinking water of so many Samoan households was a potential source of spread of vaccine-strain measles increases the importance of testing to determine exactly what was making so many Samoans sick.
Testing during an outbreak is the ONLY way to determine if the people who are showing symptoms are experiencing a wild-type measles infection, or if they are experiencing a modified measles infection as a result of vaccination.
(source)
Let’s do a little math. We’ll use the numbers for the “Disneyland Measles Outbreak” cited in the above article from the peer-reviewed medical literature. “Of the 194 measles virus sequences obtained in the United States in 2015, 73 were identified as vaccine sequences.” 73 is 37.6% of 194. If we estimate that 37.6% of the “measles” cases in Samoa were vaccine strain, how many of the 5,700 cases would be vaccine-associated measles? The answer is 2,143 vaccine-strain measles cases. However, we have to consider the difference in the health status (and drinking water) of the population of Samoa vs. the population of Southern California. When we do that, the likely number of vaccine-strain measles cases in Samoa in 2019 increases substantially.
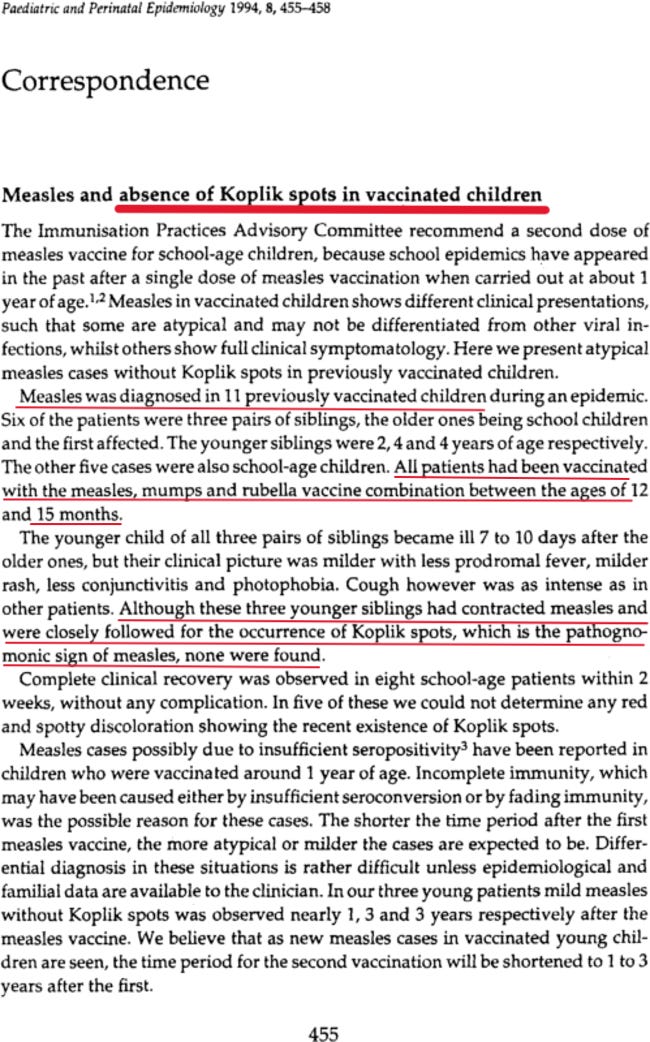
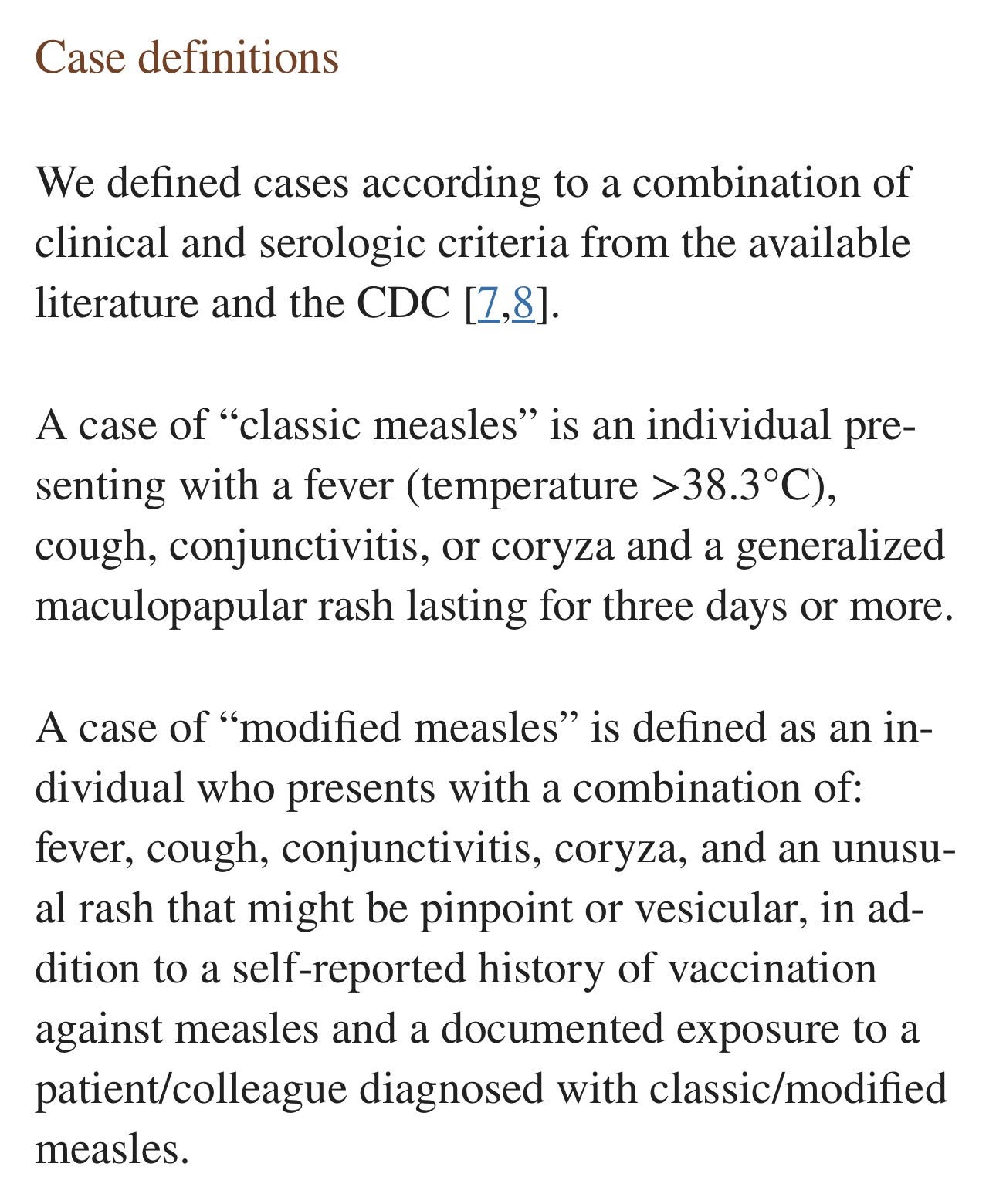
What are the differences in presentation between wild measles and vaccine-strain measles infections (aka “modified measles” or “atypical measles”)?
Here is some information from the peer-reviewed medical literature:
(source)
(source)
As these case definitions indicate, distinguishing between a wild measles infection and a vaccine-associated measles infection can be difficult. One difference that can help distinguish between the two is the presence or absence of Koplik spots. Koplik spots are almost always present in wild measles infections, and almost never present in vaccine-associated measles infections.
Meet Dr. Blessy John-Denny, a pediatrician and pediatric emergency physician who was in Samoa and treating severely ill children during the measles outbreak.
Here is what Dr. John-Denny has to say about her experience with the presentation of measles in the children she treated:
Dr. John-Denny saw no evidence of Koplik spots in the children she treated in Samoa.
What does Dr. John-Denny have to say about the overall health of the children she treated in Samoa during the measles outbreak?
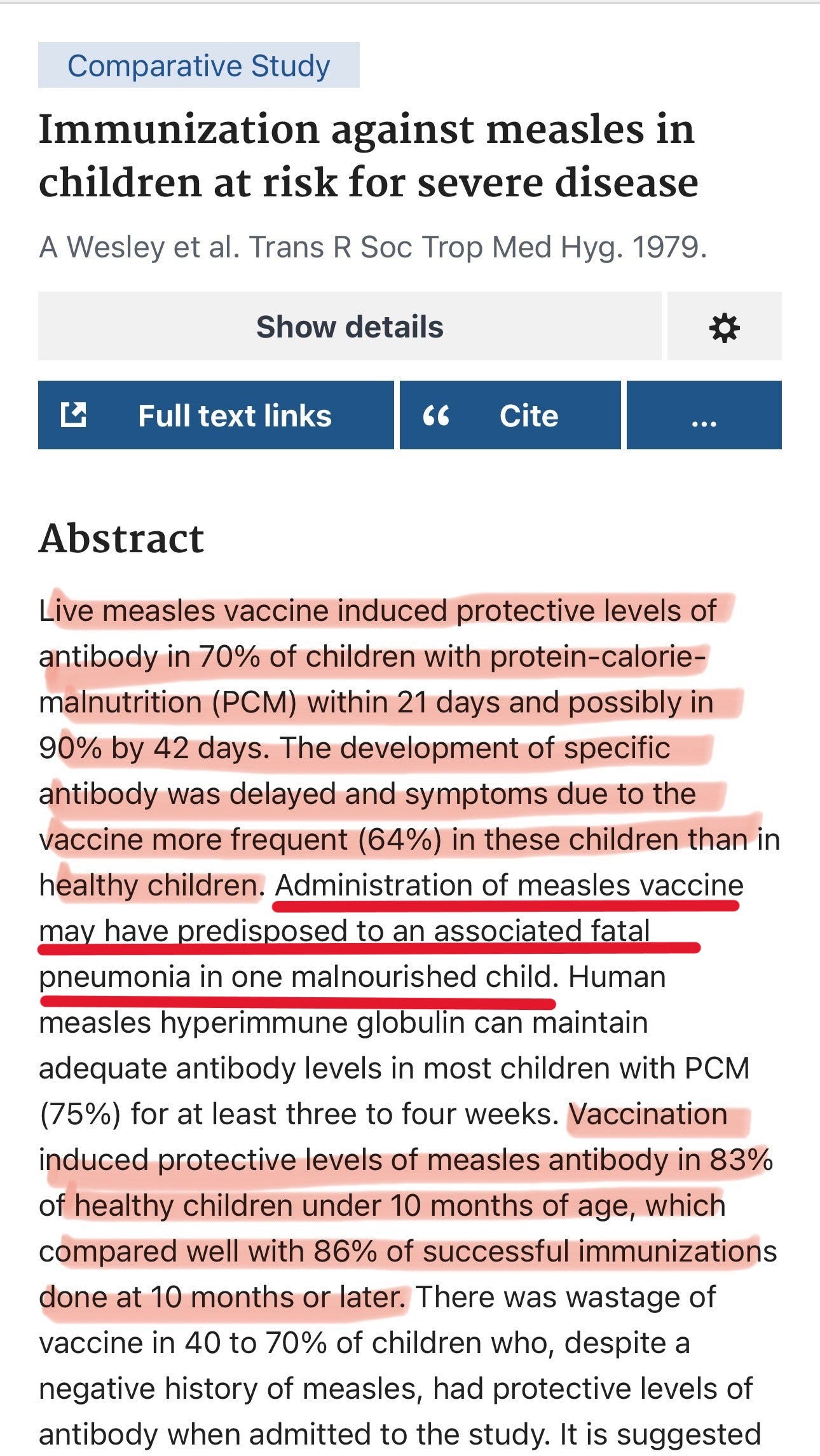
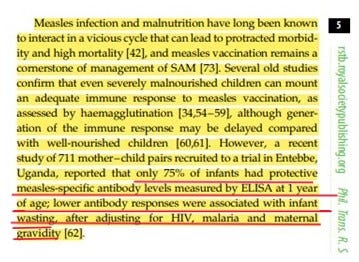
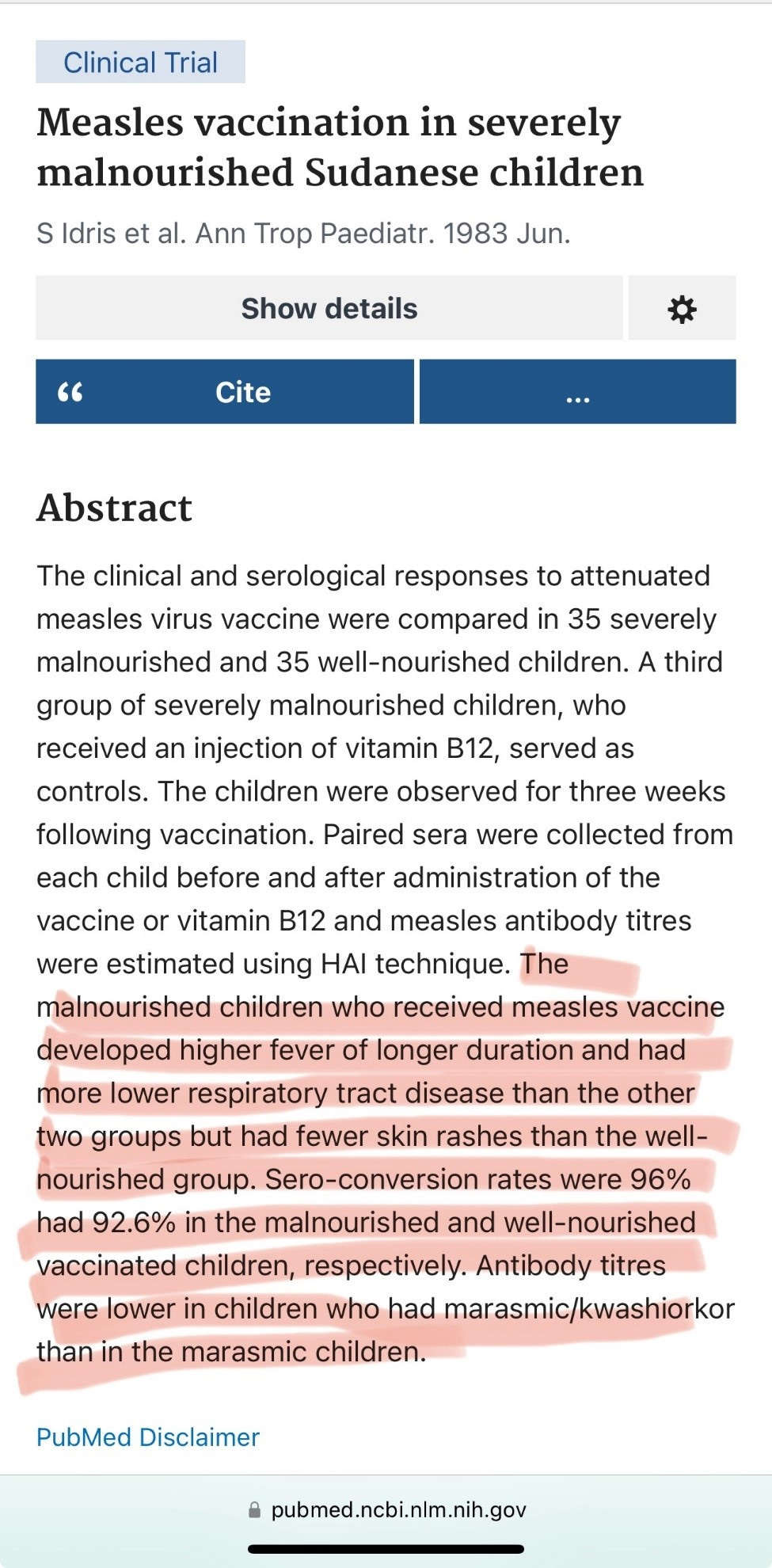
How does the response to measles vaccination differ in children who are experiencing serious malnutrition?
(source)
(source)
(source)
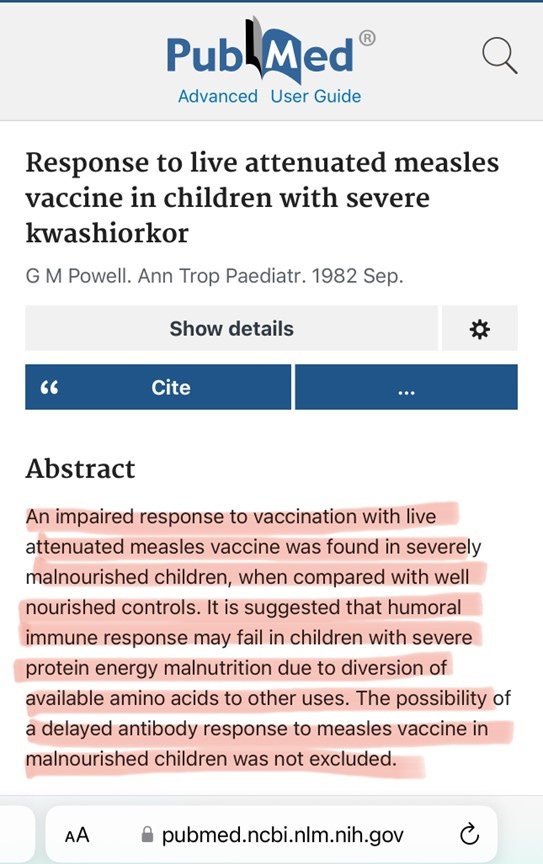
(source)
In infants and children with serious malnutrition, the response to measles vaccine is delayed, with very high rates (64%) of adverse reactions to vaccination, and 25% of infants vaccinated at six months showing no evidence of antibody protection by 1 year of age. Remember that according to the Samoan government’s health survey conducted in 2019-2020, 15.1% of Samoan children under the age of five met the criteria for stunting or wasting due to serious malnutrition.
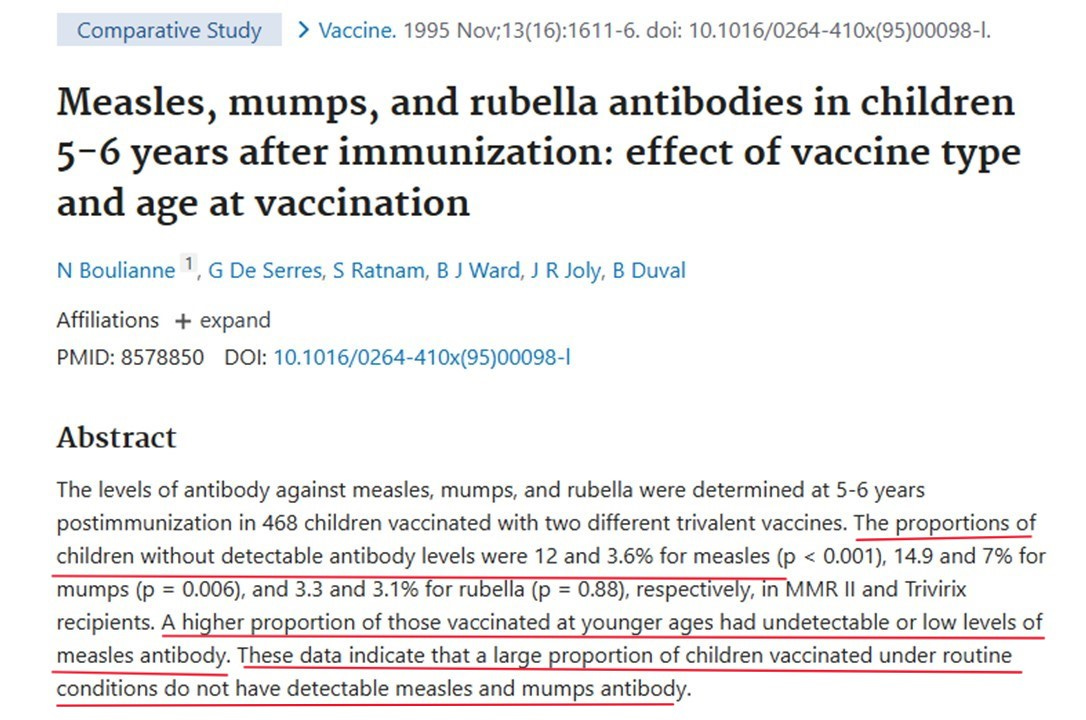
As we can see, several studies have found that the immune response of malnourished children to the live attenuated measles vaccine was significantly lower than that of their adequately nourished peers (70% vs. 83-86%), and the development of “protective immunity,” when present, was significantly delayed. Malnourished children are also far more likely to manifest serious negative reactions to vaccination, with higher fevers that persist longer after vaccination, and significantly higher rates of lower respiratory illness, including pneumonia, post-vaccination. (source)
Okay. So, now we know that severe malnutrition affects the response to live attenuated measles vaccine in multiple ways:
Lower immune response,
Delayed immune response,
Higher rate of adverse reactions and symptoms from the vaccine, including higher fevers that last longer and increased incidence of lower respiratory illness, including pneumonia,
Prolonged time to clear the (vaccine strain) virus from nasopharyngeal passages, increasing the amount of time during which the vaccinee is shedding the virus, thereby increasing the amount of time during which the vaccinee can infect others with (vaccine strain) measles.
According to the following article, vaccine-strain measles and delayed immune response does not just affect severely malnourished children. This article reports on a case of vaccine-strain measles infection that was indistinguishable from wild-type measles, 37 days post vaccination with MMR:
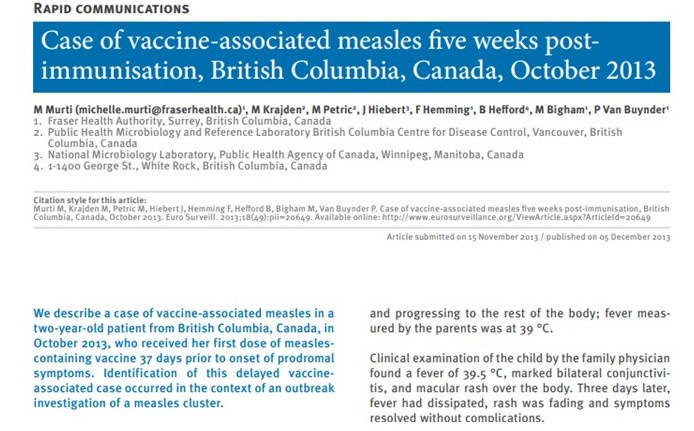
Wow. Five weeks post-vaccination. How many people does a child come in contact with over a five-week period of time?
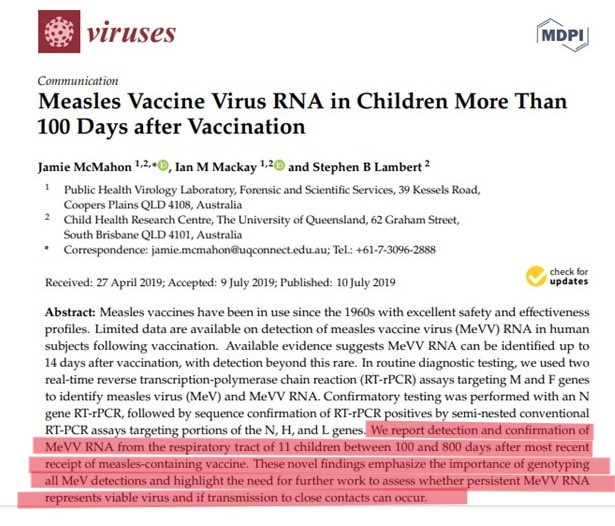
This article documents vaccine-strain measles in the respiratory tracts of vaccinated children for WAY longer than five weeks.
And… what about the effect of vaccinating thousands of children as early as six months of age, as the Samoan Ministry of Health mandated?
(source)
By now you should be coming to the conclusion that vaccinating very young children, and especially very young children who are suffering the effects of severe, acute malnutrition is a bad idea. And doing so during an active epidemic is a really bad idea.
What about Vitamin A?
You may have heard that measles-related complications like pneumonia and encephalitis are more frequent in children who suffer from vitamin A deficiency. This has been known since the 1930s and it’s the reason why the World Health Organization recommends giving vitamin A to children with measles.
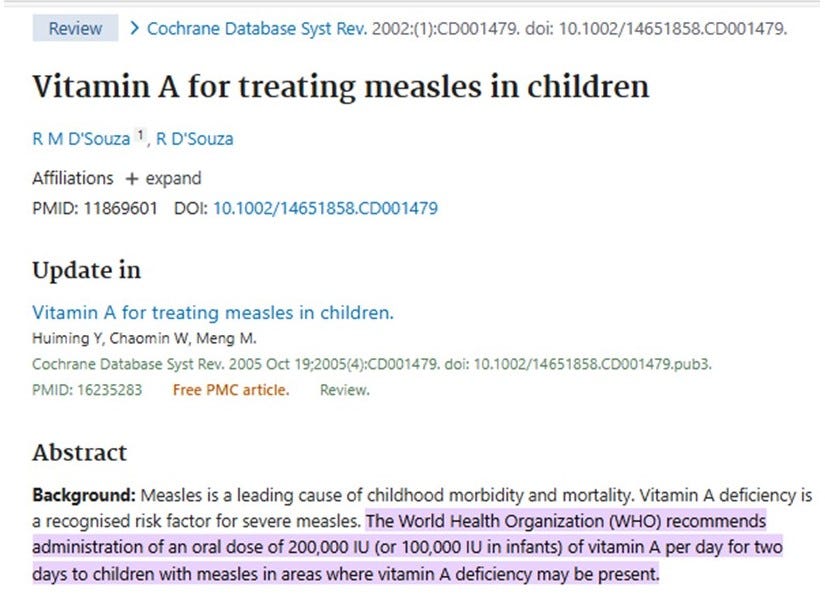
Measles vaccination ALSO CAUSES serum vitamin A levels to drop, as this study shows.
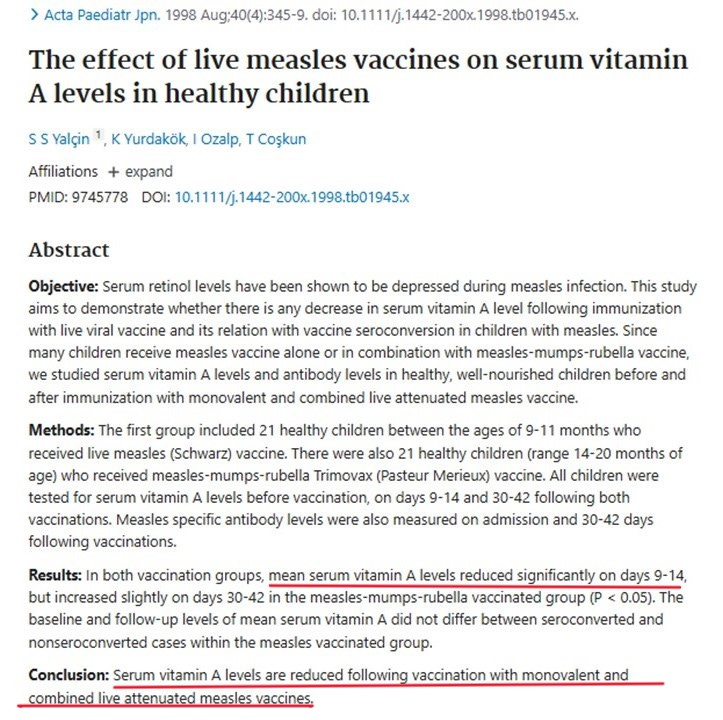
If that’s what happens to healthy children, what do you think happens to infants and children who are already seriously malnourished when they are vaccinated with the MMR? Their already low rates of serum vitamin A drop even further, which puts them at increased risk of serious complications from measles, which is particularly problematic if they are vaccinated during an active outbreak where they are more likely to be exposed to measles.
It should be noted here that during the 2019 measles outbreak in Samoa, there were activists and doctors who were advocating for the administration of Vitamin A for the children, and those people were called “conspiracy theorists” and “anti-vaxxers.” One such activist, Edwin Tamasese was arrested and charged with going against a government order because he was advocating for the use of vitamin A to prevent serious complications from measles infection.

Can someone with vaccine-associated measles spread it to others? You betcha. It happened in New York just a few years ago.

(source)
Lest you think the New York Measles Mary case was an isolated event…
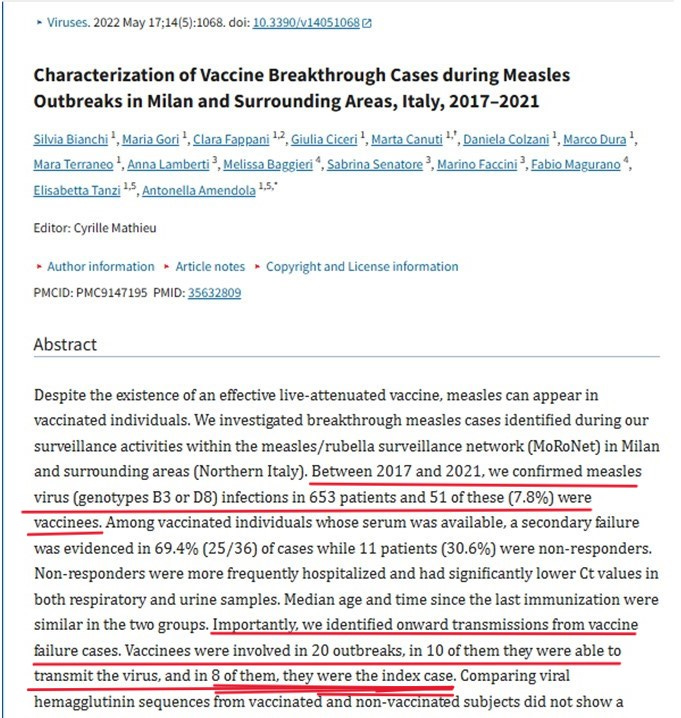
(source)
In this article, the CDC reports on an investigation into an outbreak of measles among members of the Israeli Military.
On August 6, 2017, the Israeli Defense Force Public Heath Branch (IDFPHB) was notified of two suspected measles cases. IDFPHB conducted an epidemiologic investigation, which identified nine measles cases in a population with high measles vaccination coverage. All measles patients had signs and symptoms consistent with modified measles (i.e., less severe disease with milder rash, fever, or both, with or without other mild typical measles symptoms).
And…
The review of medical records led to further evaluation of 14 patients, including vaccination history, exposure history, inquiries regarding potential contacts, and a physical examination by a general practitioner. Among the 14 patients, eight measles cases were identified in addition to the primary case, seven of which were laboratory-confirmed (Table). The median patient age was 20 years (range = 19–37 years). All patients had mild disease with rash, fever, or both and minimal or no conjunctivitis or Koplik spots, consistent with modified measles (2).
And…
Patients were residents of central Israel and served on different military bases. Four patients had documentation of receipt of 2 doses of measles-containing vaccine, four reported receiving 2 doses during childhood (with no documentation), and the primary patient had documentation of receipt of 3 doses of MMR in Ukraine, one each in 1997, 1998, and 2002.
For clarification, “the primary patient” is the index case – the one who is credited with starting the outbreak. And he had documentation of receipt of not one, not two, but THREE doses of MMR vaccine. (scratching head…) Didn’t I just read that Ukraine has one of the largest ongoing measles outbreaks? Is what happened in Samoa repeating itself in Ukraine, where they are giving THREE doses of the MMR vaccine to infants and young children, and where the living conditions, political strife, and war are having a serious negative effect on the nutritional status and immune systems of those infants and children?
What happens to severely malnourished infants and children when they are given the MMR vaccine?
Severe Acute Malnutrition (SAM) skews the immune system, lowering the Th1 response (to viruses) and increasing the Th2 response, increasing the allergic and autoimmune/inflammatory response. Children who are severely malnourished are, by definition, immune compromised, and immune compromised people should not receive the MMR vaccine, according to the vaccine manufacturer’s insert. (Note: The MMR vaccine used in Samoa is from the Serum Institute of India. I could not find the manufacturer’s insert. That vaccine is a live attenuated trivalent vaccine and is very similar to the MMRii vaccine used in the United States. This information is from the MMRii package insert.)
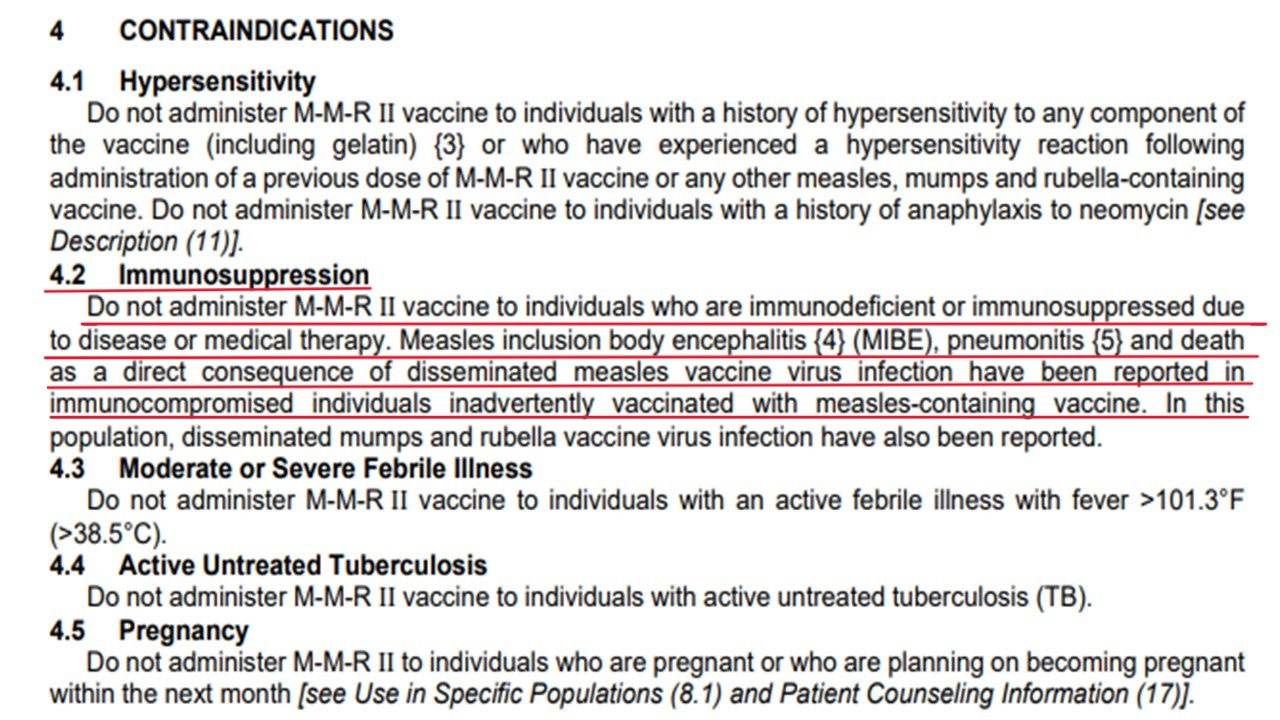
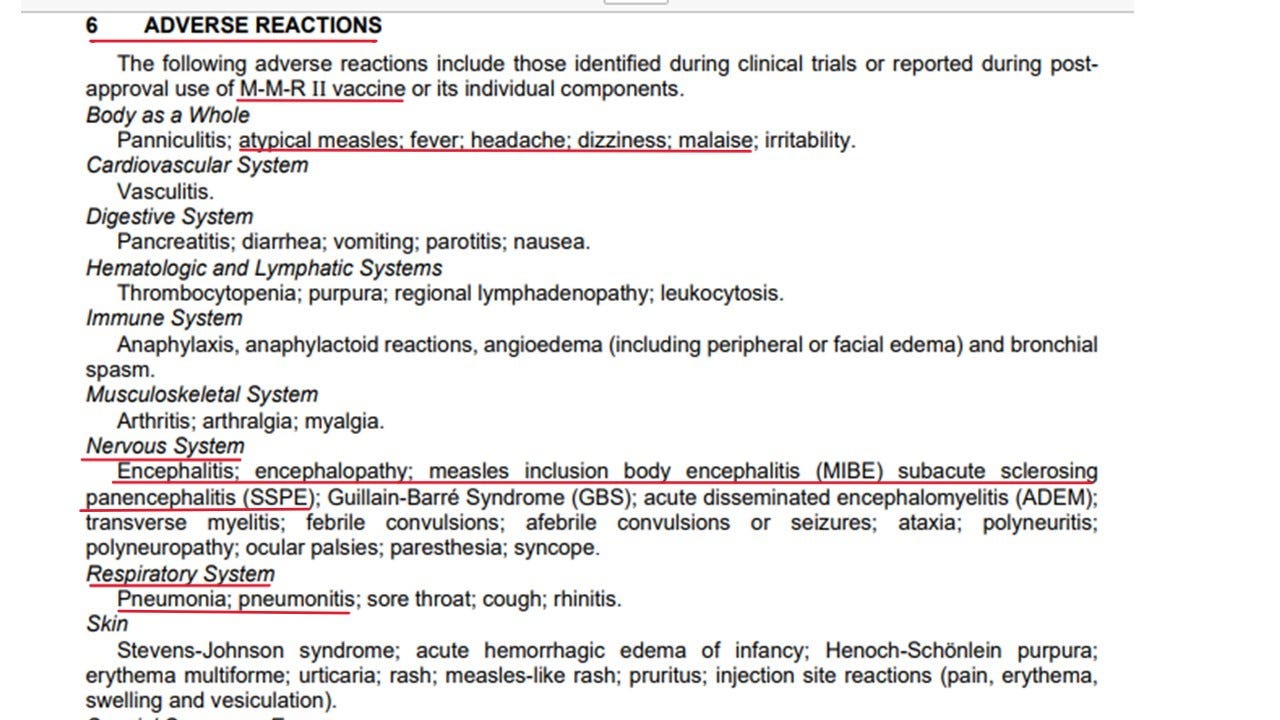
Pneumonia. Encephalitis. Remember Dr. John-Denny? Let’s see what she has to say about the unusual presentation of measles she was seeing in the children of Samoa in 2019.
Pneumonia and encephalitis are two specific adverse reactions that are noted in the vaccine-manufacturer’s inserts, and both are noted to be associated outcomes when the MMR vaccine is administered to children who are immune-compromised. It should be noted that these outcomes are not specific to the children of Samoa.
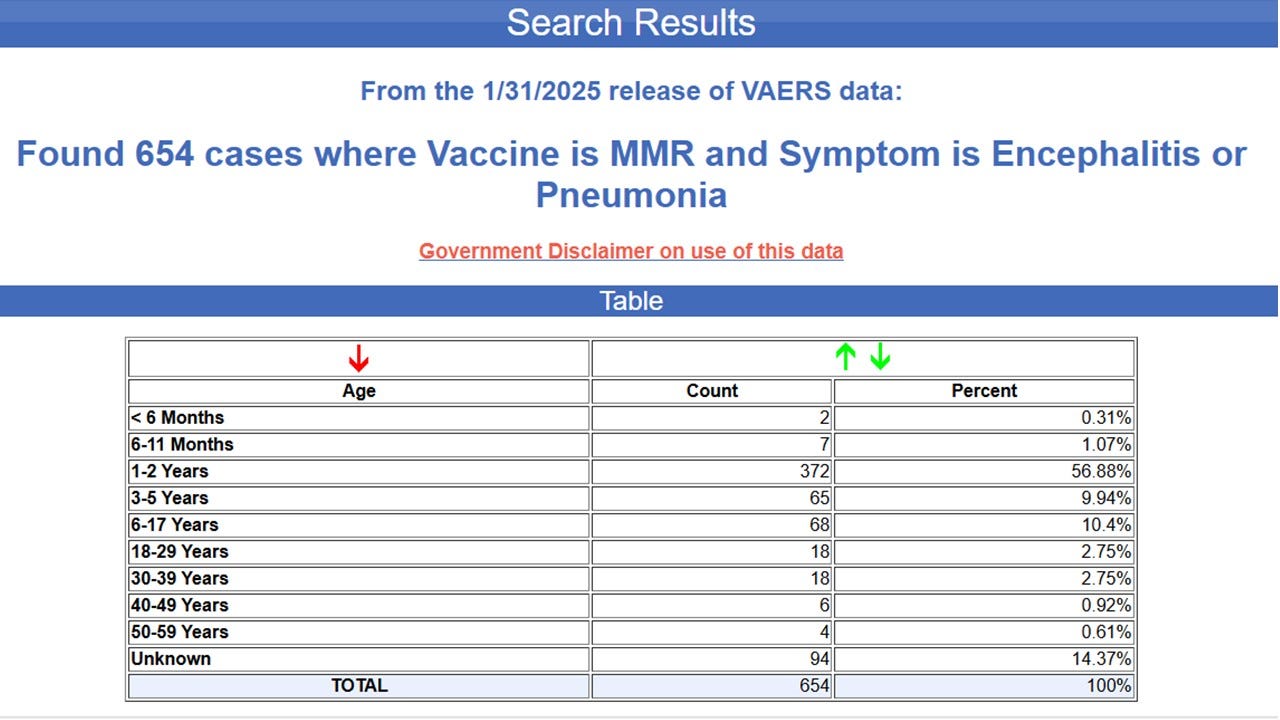
I did a quick search of the VAERS data and found the following:
I hope that as a result of reading this information, you will come to the rational conclusion that blaming RFK, Jr. for what happened in Samoa is at best, uninformed. At worst, it is a concentrated effort to hide the truth about what certainly may be high numbers of vaccine-associated deaths in infants and children in a very vulnerable population.
Thank you for reading. Please share, especially with your senators, who will be voting this week to confirm Mr. Kennedy’s appointment as the new head of Health and Human Services (HHS).
Nice report wow! Well done! How many hours went into this?
Also, speaking of encephalitis, this will really fry your noodle:
Dr. Ardis Exposes the Influenza (Flu) Shot Fraud : https://old.bitchute.com/video/QTb1GfWVy4fm/
I bet Samoa never even saw meals until the white man invaded them. But sure, go ahead and blame us anti-VAX ERS.