


You Anti-Vaxxers want to Bring Back Polio!
Let's talk about Provocation Polio and Acute Flaccid Myelitis

Anyone who has ever engaged in online debate over social media has probably been told at least once that those of us who dare to question the safety, efficacy, or necessity of all those vaccinations on the CDC’s Childhood Schedule “want to bring back polio!” Is this really a concern? In order to answer that question, we have to know a little bit about the poliovirus, the disease it causes, and the vaccines that have been credited since the 1950s with “eradicating” polio from the United States.
Thankfully, there are a couple of other people who have done amazing work in this regard: Dr. Suzanne Humphries and Neil Z. Miller.
Dr. Humphries, along with her co-author, Roman Bystrianyk, wrote an excellent book entitled, “Dissolving Illusions: Disease, Vaccines, and the Forgotten History.” I highly recommend buying a copy or two. Once you read Dissolving Illusions, I predict you will want to share it with others you love. You won’t want to give up your copy, so having an extra on hand to share is a really good idea. This video is a good sample of Dr. Suzanne’s research findings regarding “the disappearance” of polio.
Neil Z. Miller is a formidable force in the world of vaccine research. He is the Director of ThinkTwice Global Vaccine Institute and has been a prolific researcher for more than thirty years. Mr. Miller has thoroughly researched the history of the polio vaccine in his extremely well-cited article, The polio vaccine: a critical assessment of its arcane history, efficacy, and long-term health-related consequences.
Reading through just these two resources (the polio chapter of Dissolving Illusions and Mr. Miller’s article on the history of the polio vaccine) will leave you more informed than any doctor, nurse, or epidemiologist on the planet, unless of course they have also dug really deeply into the truth about the polio vaccine.
The polio vaccine is the foundation on which the modern day vaccine program was built.
Of all the vaccines and all the childhood infections they are said to prevent, polio is the one that most people think of as demonstrating the success of the vaccine program. Is it because the vaccine has truly been that successful? Or is our perception of the polio vaccine the result of a carefully crafted public relations campaign undertaken by certain United States government entities in order to obfuscate and deceive the public?
When the polio vaccine was first licensed in 1955, the incidence of paralytic polio increased.
From Mr. Miller’s report:
When national immunization campaigns were initiated in the 1950s, the number of reported cases of polio following mass inoculations with the killed-virus vaccine was significantly greater than before mass inoculations, and may have more than doubled in the U.S. as a whole. For example, Vermont reported 15 cases of polio during the one-year report period ending August 30, 1954 (before mass inoculations), compared to 55 cases of polio during the one-year period ending August 30, 1955 (after mass inoculations) - a 266% increase. Rhode Island reported 22 cases during the before inoculations period as compared to 122 cases during the after inoculations period - a 454% increase. In New Hampshire the figures increased from 38 to 129; in Connecticut they rose from 144 to 276; and in Massachusetts they swelled from 273 to 2027 - a whopping 642% increase.

Citation for the quote and figure above, here.
That first polio vaccine, the Salk inactivated polio vaccine, was an injected vaccine that was supposed to contain the killed poliovirus, but something went awry, and within a short time of its introduction, the problems were so glaringly apparent that the vaccine’s licensure was pulled, and mass-vaccination campaigns halted.
In April 1955 more than 200 000 children in five Western and mid-Western USA states received a polio vaccine in which the process of inactivating the live virus proved to be defective. Within days there were reports of paralysis and within a month the first mass vaccination programme against polio had to be abandoned. Subsequent investigations revealed that the vaccine, manufactured by the California-based family firm of Cutter Laboratories, had caused 40 000 cases of polio, leaving 200 children with varying degrees of paralysis and killing 10. (source)
The problem was that the formaldehyde used in the vaccine manufacturing process did not actually kill the poliovirus. Many children who received the shot developed polio, became paralyzed, and even died - as a result of the vaccine.
In the late 1950s, Albert Sabin was working to bring an oral polio vaccine to market. His live, attenuated polio vaccine underwent clinical trials in various countries between 1958 and 1960 and was ultimately licensed for use in the United States in 1961. It was believed that the oral polio vaccine would be more effective, particularly because it would protect the gut (since it was taken by mouth and swallowed) more efficiently than an injected vaccine. This seemed like a good hypothesis, since the gastrointestinal tract is where the poliovirus lives and replicates.
The problem was, and still is, that poliovirus is not the only thing that causes paralytic poliomyelitis. The inflammation in the central nervous system that leads to paralysis which is indistinguishable from paralytic polio can be caused by multiple different viruses. It can also be caused by pesticides and the evidence is abundant that many of the cases diagnosed as paralytic polio in the 1940s through the 1960s were the result of DDT poisoning. Heavy metal poisoning can also cause “paralytic polio,” and in mid-century America, arsenic toxicity was yet another source of paralysis which could not be differentiated from paralytic polio that was caused by poliovirus.
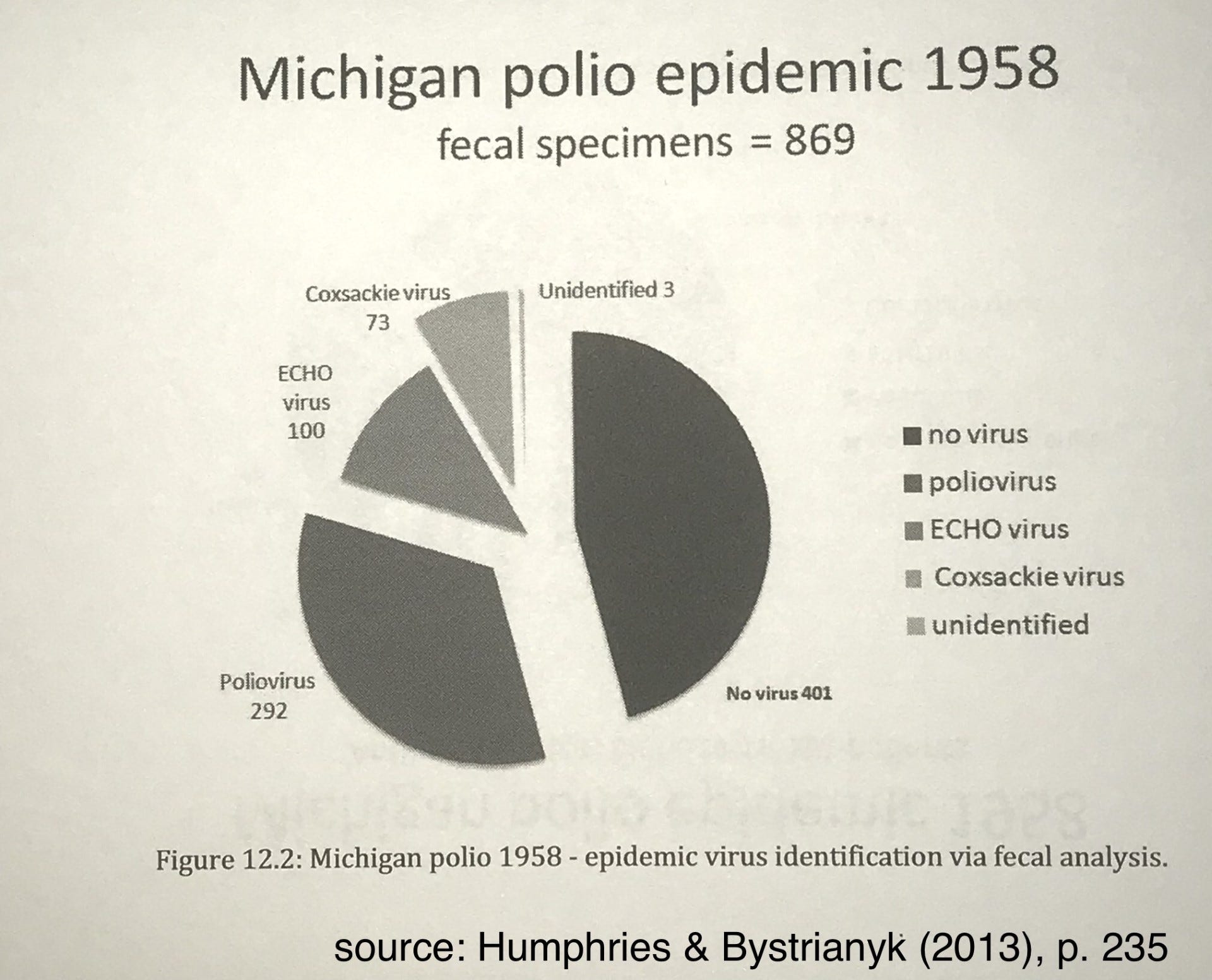
Review of the outcome of fecal studies conducted during a significant polio outbreak in Michigan in 1958 illustrates clearly that even if the polio vaccine (which contains three strains of poliovirus), eradicated 100% of those cases caused by actual poliovirus, it could not possibly have eradicated all cases of what was called “polio,” since only 33.6% of the 869 cases in that outbreak were actually found to be associated with poliovirus. The other two-thirds of the cases were caused by other viruses, or no known associated virus, and therefore, could not have been prevented by the vaccine, no matter how “safe and effective” it was advertised to be.
After the roll-out of the live oral polio vaccine it quickly became the darling of the vaccine program, and virtually every child in the United States was vaccinated with Sabin’s sugary cocktail multiple times before entering school. It wasn’t until many years later that problems became known about the contamination of the vaccine, which included SV40, a simian virus that is known to be carcinogenic, and which has been found in all different kinds of tumors, and which is also now known to be passed from parent to child in utero. SV40 originated in African Green Monkeys, the kidneys of which are used in the manufacture of the polio vaccine. Once again, I highly recommend reading Neil Miller’s article, The polio vaccine: a critical assessment of its arcane history, efficacy, and long-term health-related consequences. The contamination with SV40 is just one of the many issues of concern with this vaccine, which Mr. Miller’s research reveals.
Given that only a percentage of the paralytic polio cases were actually associated with poliovirus, how could the vaccine have eradicated polio? It didn’t. As noted previously, after the vaccines were introduced, the cases of paralytic polio increased. They had to do something to make that go away, so they created new diagnostic labels for things that USED to be called polio.
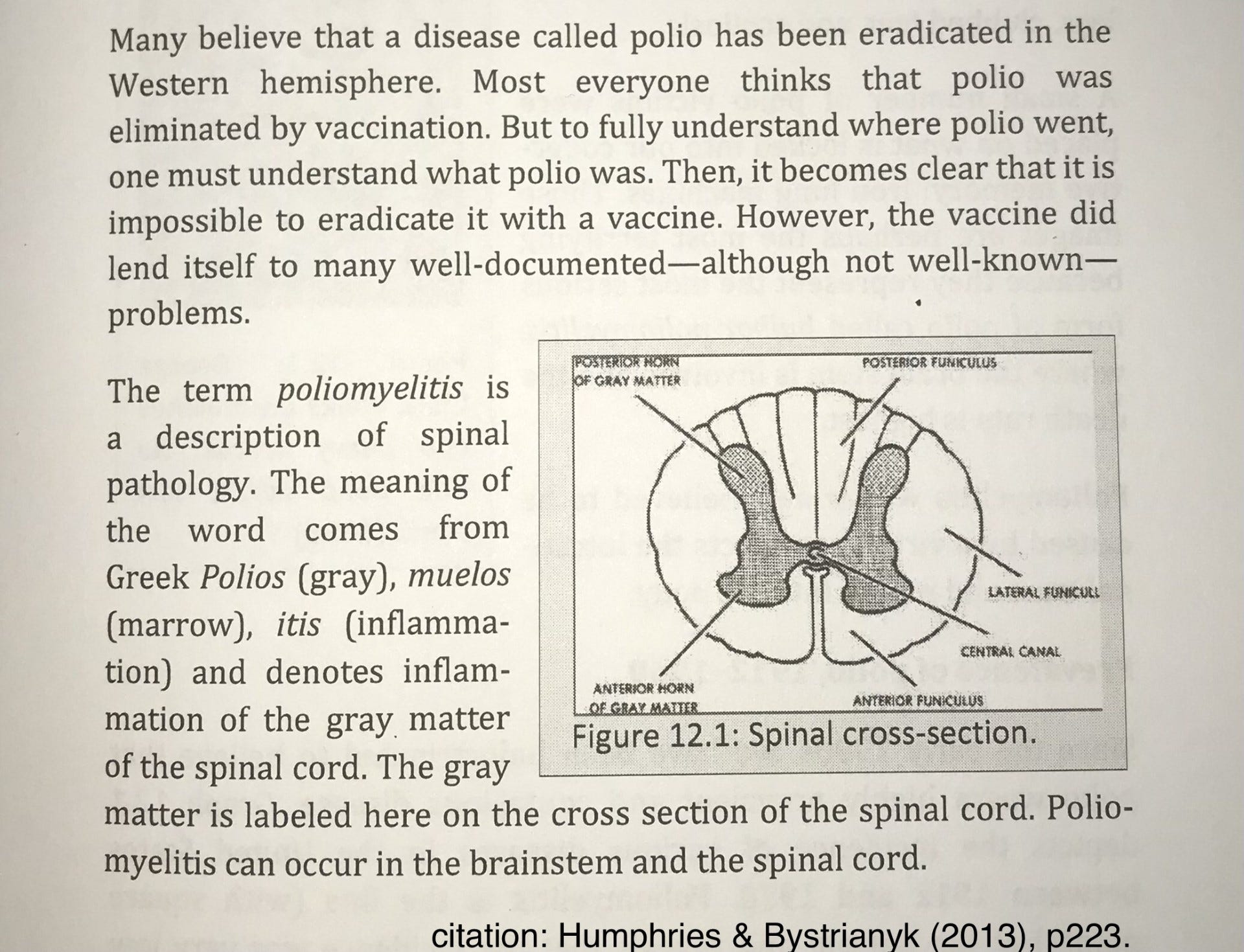
After the vaccine, there was a concerted effort to distinguish cases with poliovirus from cases without it. This was not a concern prior to 1958 when many diseases common today hid behind the name poliomyelitis. Transverse myelitis, viral or aseptic meningitis, Guillain-Barre syndrome (GBS), chronic fatigue syndrome, spinal meningitis, post-polio syndrome, acute flaccid paralysis (AFP), enteroviral encephalopathy, traumatic neuritis, Reye’s Syndrome, etc, all could have been diagnosed as polio prior to 1958. (source: Humphries & Bystrianyk (2013), p. 234.)
One of the most important things that happened was that prior to the rollout of the vaccine, ANY paralysis, of ANY severity, and ANY duration, was labeled “paralytic polio.” After the vaccine, the diagnostic criteria were changed, and in order to receive a “paralytic polio” diagnosis, the paralysis had to last at least 60 days. This one change had the effect of wiping out many cases of “paralytic polio,” since in a high percentage of paralysis cases, improvement occurred before that 60-day mark and the patient no longer suffered from paralysis.
The oral polio vaccine had a particularly nasty side effect. Because it was a live viral vaccine, it could not be given to people with compromised immune systems because it could give them polio. Because the virus replicates in the gastrointestinal tract, live polio virus was found in the feces of children who had been recently vaccinated. Cases of vaccine strain polio started happening in family members who were coming in contact with polio while changing diapers of vaccinated children. This is an ongoing problem in places where the live oral polio vaccine is still in use, and it’s particularly problematic in places where there is inadequate sewage treatment and a lot of poverty.
Because of problems with the oral polio vaccine, the U.S. stopped giving it in 2000 and switched back to a “killed” polio virus vaccine that is injected - the Inactivated Polio Vaccine (IPV). Of course, the mantra for this one is “Safe and Effective.” Just as it was for the first two, which were pulled because they were not safe or effective.
Given that there are many problems with the oral polio vaccine and given that the first “inactivated” polio vaccine was not really inactivated and resulted in many cases of paralysis and death, IF one knows the history, it can be easy to understand why one might have questions.
But those questions are not allowed to exist.

Have you ever heard of The Federal Register? It’s basically the newspaper for the United States Federal Government, where they publish new rules and regulations, and changes to existing rules and regulations. In 1984, there was an article published in the Federal Register, in which they were discussing concerns about the safety of the polio vaccine. It was noted that in the clinical trials, not all of the safety regulations had been followed before the vaccine was licensed. Rather than going back and making sure those steps were adequate to ensure safety, TPTB decided that doing so would be too restrictive on the manufacturers and since the vaccine was already in use and being given to millions of children, it would be disruptive to the program if this little safety glitch were to come to light. So, they not only decided to change their requirements after the fact, they also decided to forgo the established procedure of letting the public know what had happened and why they were changing the rules. They just slid this one in without telling anyone. And they did it to protect the program.
From the article, on page 23004:
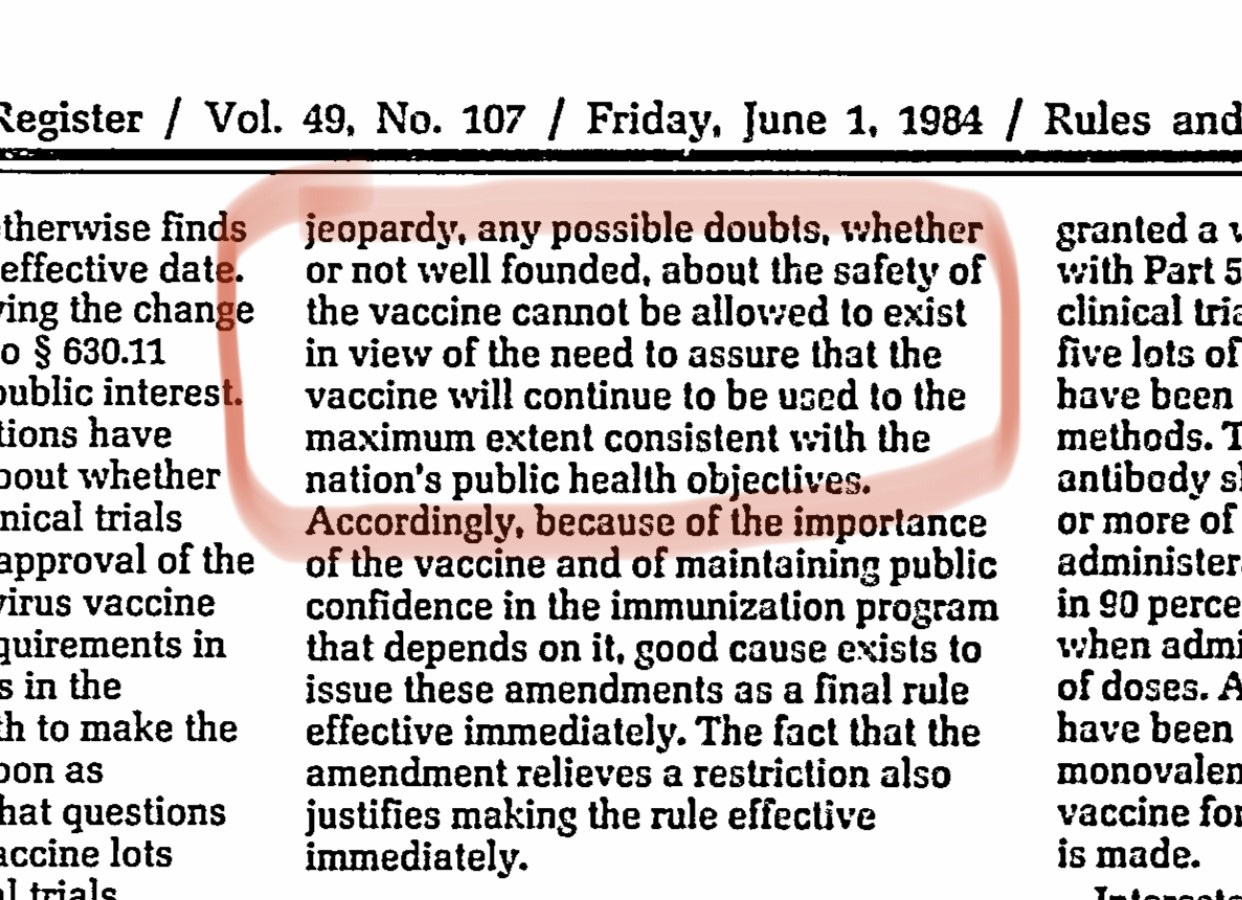
If reading that paragraph doesn’t result in a WTF moment for you, we are not the same. “Any possible doubts CANNOT BE ALLOWED TO EXIST. Regardless of “whether or not well founded.” Given the absolute denial that is currently going on with the COVID-19 shots, and the absolute denial of ANY association between vaccines and autism, it should be pretty clear to anyone who is paying attention that those people who are making decisions about the health and well-being of our children and grandchildren have one concern and one concern only:
PROTECTING THE PROGRAM.
As I was thinking about this last night, it suddenly occurred to me that something very strange happened during the summer of 2022. In July of 2022, a case of polio was identified in an unvaccinated man in Rockland County, New York. In the first news reports, much was made of the fact that the man was unvaccinated - an attempt to blame “anti-vaxxers” for the outbreak. Soon, though, when it became clear that the source of the “outbreak” was the oral polio vaccine, things got pretty quiet. News reports emphasized that the vaccine is “safe and effective” and the best way to protect yourself from this vaccine-strain polio outbreak is… you guessed it. More vaccines. It’s enough to make your head spin. Then something else happened. While New York’s governor issued a state of emergency, the news stopped reporting on the outbreak.
Anyone who recalls the 2015 “Disneyland Measles Outbreak” and how long that fiasco went on might be scratching their head wondering why the news reports on this POLIO OUTBREAK fizzled out so quickly. The answer to that is simple. It happened during the COVID-19 pandemic, when our nation’s leaders and health “authorities” were (still are) trying to convince everyone to take the COVID-19 shot. With all of the published reports of injury and death from the shot and given that COVID-19 infection has a less than one percent death rate for the vast majority of people, TRUST in the “safety and efficacy” of the shot is paramount. That means TRUST in the vaccine program has to be paramount. The finding of vaccine-strain polio in sewage samples from multiple counties in New York is problematic. If people start researching the polio vaccine, and if they learn about all the problems with the polio vaccine, including the fact that their questions or doubts “cannot be allowed to exist,” that could be an issue that would affect their willingness to accept other vaccines - including the COVID shot.
In addition to the trust problem, there is another issue… If polio is found in the wastewater of multiple counties in New York, and only one case of polio was actually identified, does that mean that polio is not the horrible crippler and killer of children that we have been led to believe? Yes. That’s exactly what it means.
When someone accuses me of wanting to bring back polio, my first response is to educate that person on the truth about the “horrors” of polio. I do that by going to the CDC and WHO.
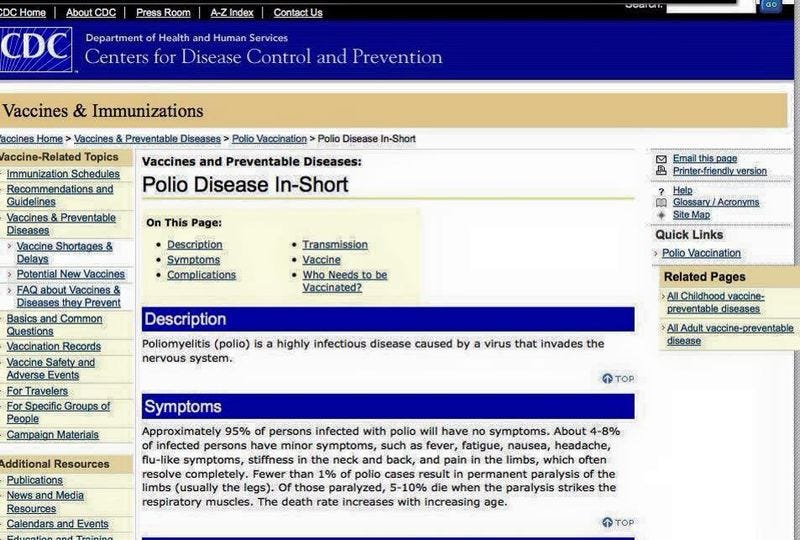
Note that under “Symptoms” the CDC states, “Approximately 95% of persons infected with polio will have no symptoms.” I screen shot this information several years ago - probably around 2012-2013. The CDC has since changed the information and now states that about 75% of people have no symptoms and about 25% of people experience mild, flu-like symptoms.
From the CDC page, What is Polio:

Gee. That’s a bit different from what most people think of when they think of polio. This is what we’ve been conditioned to think of:

The CDC goes on to state that somewhere between 1 in 200 and 1 in 2000 people infected with the poliovirus will experience some level of paralysis and between 2-10% of those paralyzed will die, because the virus paralyzes the muscles necessary to breathe.
This is what the World Health Organization (WHO) has to say about polio:
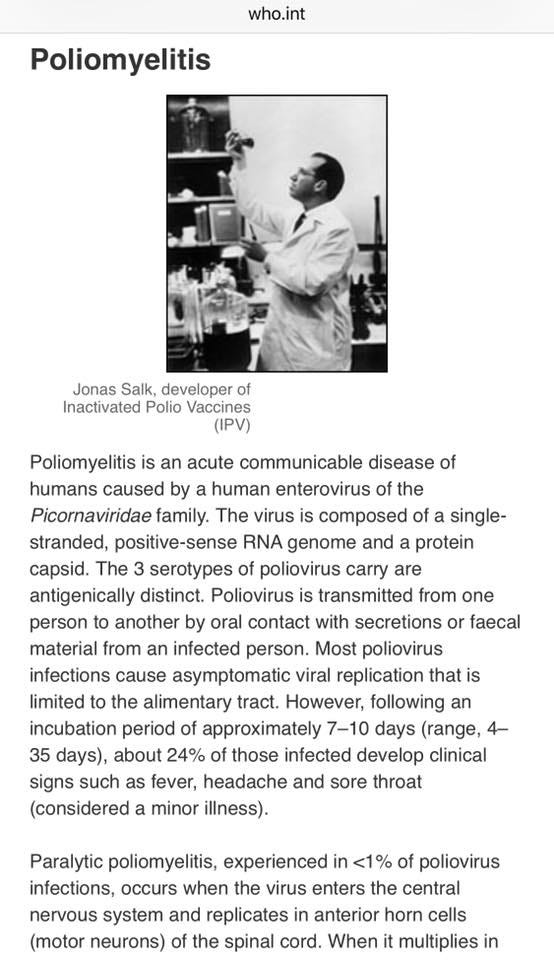
Pretty consistent. Both the CDC and WHO state that most people who contract polio have zero symptoms. Of those who do have symptoms, most of them have mild, flu-like symptoms, not at all unlike COVID. Or flu. Or a cold, allergies, or sinus infection.
So, my response to those who accuse me of wanting to bring back polio is, “How do we know it’s gone? If 99% of people who contract polio have either zero symptoms, or mild, flu-like symptoms, how would we even know if polio had been eradicated? When is the last time you went to your doctor with mild, flu-like symptoms, and asked to be tested for polio?”
Those people who lived through the mid-1900s in the United States remember the fear associated with polio. Children were being paralyzed. Images of the iron lung are burned in their memories. FYI… the iron lung has evolved and is now what we know as the ventilator. It’s not gone. It’s still being used everywhere and one of the things it is used for is when a patient has Transverse Myelitis. Ventilators are also used in patients who have been diagnosed with Acute Flaccid Myelitis/Paralysis, which is a type of Transverse Myelitis. Remember, both of these diagnostic labels were created after the polio vaccine was developed and had the effect of making it look like the vaccine eradicated polio. It didn’t. Since we know that poliovirus is actually quite benign in the vast majority of people, and since we know that other things (viruses, pesticides, heavy metals) can cause paralysis that LOOKS like what we have been taught to believe is polio, it is worth spending some time talking about those other things.

Polly Tommey is currently traveling the country and collecting the testimonies of families whose children have been harmed by vaccination. Please watch this brief video so you can experience just a small snippet of what is happening to America’s children.
The children in the video above were injured by vaccination. If this had happened to them in the 1940s or 1950s, they would have been diagnosed with “polio.” In 2014, 2016, and 2018, there were multiple cases of Acute Flaccid Myelitis in the news. It was called “the mysterious polio-like illness” affecting children. AFM was initially attributed to enterovirus D68, which had been circulating in the environment and which was found in approximately 20% of children affected with AFM. At the time (2014) the CDC initially pointed doctors in the direction of EV-D68, but then, suddenly, after a single case was found to have been associated with cytomegalovirus, the CDC stopped advising doctors to test for EV-D68. I wondered why that could be, unless the CDC was wanting to deflect attention AWAY from EV-D68 for some reason. One possible explanation for the CDC’s shift away from EV-D68 is because it is used in the manufacture of the inactivated polio vaccine currently licensed for use in the United States. Interestingly, Coxsackie virus has also been implicated in AFM, and… you guessed it… it’s also used in the manufacture of the polio vaccine currently being used.
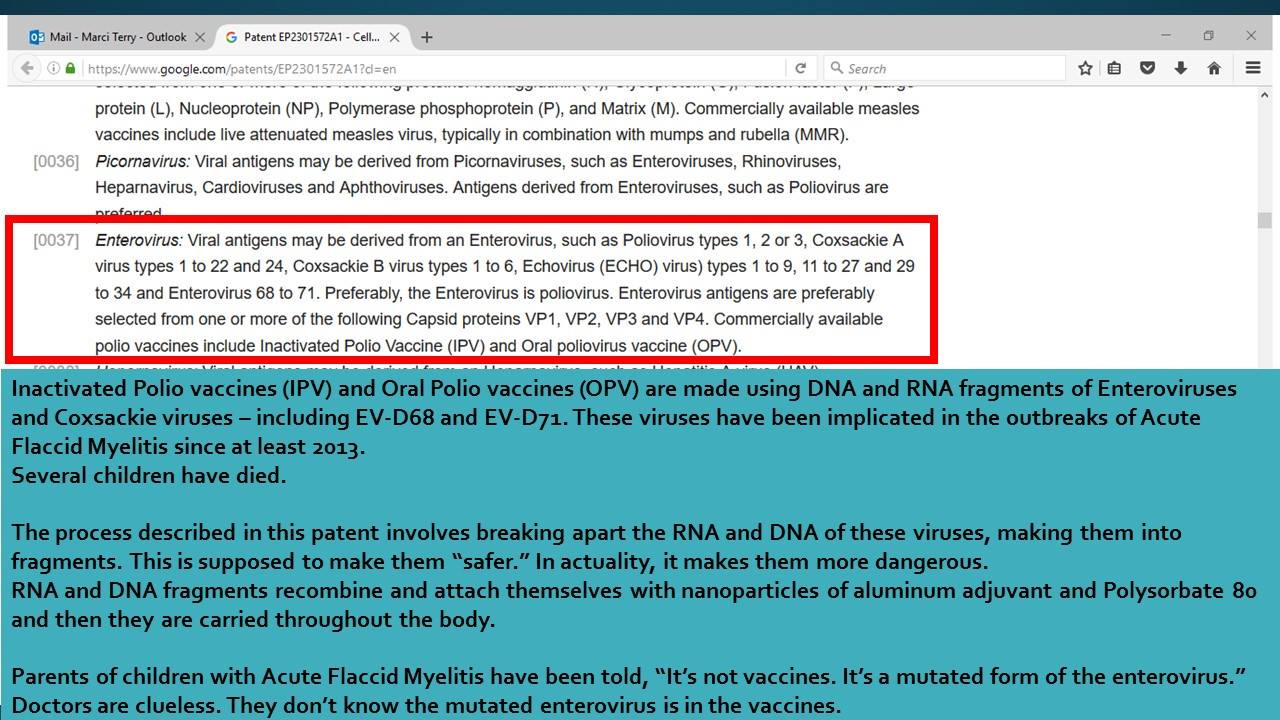
Is the presence of these viral particles in the vaccine responsible for causing AFM? Is it a possible contributing factor? There is no way to know because there haven’t been any studies done. And there won’t be. Remember, it’s all about protecting the program, and any doubts, whether or not well-founded, cannot be allowed to exist. They will never do those studies because if they found what is suspected, it would tank the program, and the program is of primary importance.
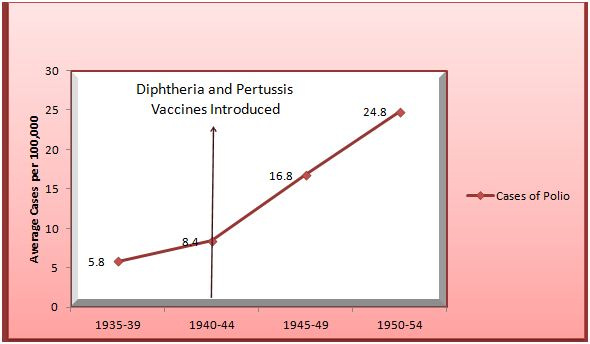
The evidence that routine childhood vaccinations can be a cause of paralytic poliomyelitis goes back a long time. The following graph is from Neil Miller’s work:
Acute Flaccid Myelitis and Routine Childhood Vaccinations: This is Nothing New
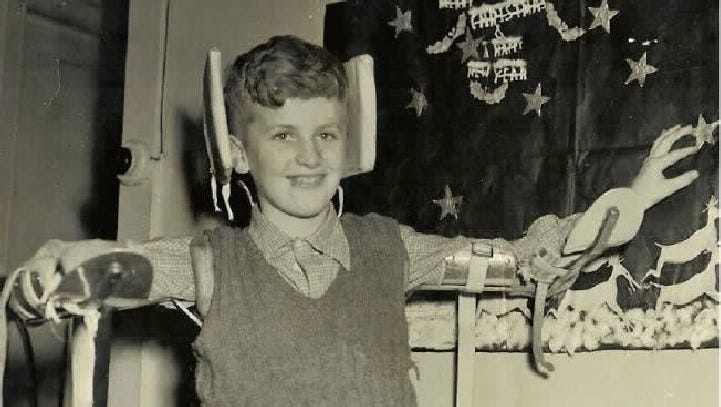
The photograph above is of Kevin Norbury, taken when he was recovering from polio. Kevin is from Australia. He became paralyzed with polio in 1951, at the age of 10. Kevin’s paralysis began shortly after he was vaccinated against diphtheria, and the paralysis began in the same arm where he received the vaccine. Kevin spent several years in a hospital for disabled children, and as an older adult, he still lives with the remnants of polio. It wasn’t until many years later that Kevin learned that the Australian government had known about a connection between routine childhood vaccinations and increased risk of paralysis from polio, AND they covered it up.
Kevin has written a memoir entitled, The Improbable Reporter. He was interviewed by Andrew Rule of the Sunday Sun Herald and his story was published March 12, 2016.
Here is a quote from the article:
Dr Bertram McCloskey no doubt saved many lives, maybe even Norbury’s own. But it wasn’t until the adult Norbury dug up a report McCloskey published in a medical journal that he heard of a likely link between the 1950s polio epidemic and inoculation against whooping cough and the deadly disease diphtheria, which once killed tens of thousands of children a year. His report in The Lancet makes disturbing reading, even today,” Norbury begins. McCloskey had noticed that 211 of 340 polio cases in Victoria in six months were children who had been inoculated — and that the more recent the injection, the more likely it was they had developed polio. Even more pointedly, the polio paralysis was more severe in whichever arm the child had recently had injected. This rang alarm bells with Norbury. Because of problems with the primitive syringes then used, he’d been given a double dose of diphtheria vaccine, he says, only weeks before the paralysis hit him. The veteran journalist would ferret out facts hidden from his parents and others when he was a child. He discovered that McCloskey had reported his misgivings to the Victorian chief health officer, the heads of the Commonwealth Serum Laboratories and the head of the Infectious Diseases Hospital. They agreed there was a link between school injections and polio. In fact, the Medical Journal of Australia advised against injecting school-aged children in areas where polio was breaking out. Experts apparently suspected that children’s immune systems were temporarily weakened by the vaccines, making them vulnerable to polio. So what happened? Because of fears of a backlash against immunisation, the authorities buried McCloskey’s report. People in high places thought that the increased risk of hundreds of children getting polio was better than postponing diphtheria vaccinations.
The connection between childhood vaccination and paralysis has been known since the polio outbreaks in the 1940s and 1950s, and the knowledge was not confined to Australia. It also happened in the United States, Canada, Germany, Italy, France, and England. There is a very good article in The Lancet, entitled Polio Provocation: Solving a Mystery with the Help of History. In the article, the author, Stephen Mawdsley reveals some very interesting facts about the association between vaccination with diphtheria, tetanus, and pertussis, and the increased risk of paralytic polio in recently vaccinated children.
From the Lancet article:
… it was not until the end of World War II that injection-induced polio emerged as a public health concern. The application of epidemiological surveillance and statistical methods enabled researchers to trace the steady rise in polio incidence along with the expansion of immunisation programmes for diphtheria, pertussis, and tetanus. A report that emerged from Guy’s and Evelina Hospitals, London, in 1950, found that 17 cases of polio paralysis developed in the limb injected with pertussis or tetanus inoculations. Results published by Australian doctor Bertram McCloskey also showed a strong association between injections and polio paralysis. Meanwhile, in the USA, public health researchers in New York and Pennsylvania reached similar conclusions. Clinical evidence, derived from across three continents, had established a theory that required attention.
Mawdsley goes on to discuss the theories about the mechanism behind polio provocation, which included the hypothesis that the act of piercing the skin during injection drove the polio virus into deep tissue, and from there, into the central nervous system, where it led to paralysis and sometimes, death.
What did the United States Health Authorities do???
Mawdsley writes:
The impressive volume of literature on polio provocation by the 1950s fueled changes in health policy. US health organisations and charities, including the National Foundation for Infantile Paralysis, the American Academy of Pediatrics, and the American Public Health Association, accommodated the possibility of polio provocation and encouraged health professionals to avoid “indiscriminate” injections and “booster shots” during epidemics. In New York City, child health stations were closed and laws mandating paediatric vaccinations before school attendance were relaxed. Most health professionals reformed their immunisation practices and accepted that seasonal factors and cycles of disease were important to consider before immunising children.
In the 1940s and 1950s, the mechanisms of provoked polio were hypothetical. They didn’t stay hypothetical. In an article from 1998, published in the Journal of Virology, researchers reported their findings, which confirmed the suspicions of nearly half a century earlier, writing:
Skeletal muscle injury is known to predispose its sufferers to neurological complications of concurrent poliovirus infections. This phenomenon, labeled “provocation poliomyelitis,” continues to cause numerous cases of childhood paralysis due to the administration of unnecessary injections to children in areas where poliovirus is endemic. Recently, it has been reported that intramuscular injections may also increase the likelihood of vaccine-associated paralytic poliomyelitis in recipients of live attenuated poliovirus vaccines. We have studied this important risk factor for paralytic polio in an animal system for poliomyelitis and have determined the pathogenic mechanism linking intramuscular injections and provocation poliomyelitis. Skeletal muscle injury induces retrograde axonal transport of poliovirus and thereby facilitates viral invasion of the central nervous system and the progression of spinal cord damage. The pathogenic mechanism of provocation poliomyelitis may differ from that of polio acquired in the absence of predisposing factors.
The viruses that have been associated with the more recent hospitalizations of children from acute flaccid myelitis include Enterovirus D68, Coxsackie virus, and Cytomegalovirus. The viruses are different (though similar), but the mechanism is the same: piercing the skin and driving what is otherwise a benign infection into skeletal muscle and from there, into the spinal column. Interestingly, there is some suspicion that the live viral flu vaccine (FluMist) may also be associated with AFM, particularly when it is given along with the inactivated polio vaccine and or other injected vaccines. A few years ago, FluMist was pulled, ostensibly because it had such a low efficacy rate (generally around 3%) against influenza. Having low efficacy is not typically a reason for pulling a vaccine once it’s been approved, so those of us who have suspicious minds were left wondering what the actual reason might be. The rates of AFM went down when FluMist was unavailable. Then it was reintroduced, and the AFM rates went up again. Of course, correlation does not equal causation (insert eye-roll here), and of course, there will never be a study to actually look and see if FluMist and AFM are linked, because… protecting the program is paramount.
There are some doctors who remember provocation polio. One of those doctors is Alan S. Cunningham, M.D., a retired pediatrician. Dr. Cunningham’s concerns were published in The BMJ, in January of 2015.
Dr. Cunningham wrote:
Since August 2, 2014 our Centers for Disease Control has received reports of 107 cases of ‘acute flaccid myelitis’ (AFM), a polio-like illness in children in 34 states. During the same interval there have been 1153 cases of respiratory illnesses associated with enterovirus D-68 (CIDRAP News 1/16/15. CDC update 1/15/15. Catherine Saint Louis, NY Times 1/13/15). AFM affects motor neurons in spinal cord gray matter, resulting in asymmetrical limb weakness; 34% of patients have cranial nerve motor dysfunction. Median age of patients is 7.6 years/range: 5 months-20 years (MMWR 63: 1243–January 9, 2015). So far only one child has fully recovered. EV-D68 is a suspected cause but, thus far, no viruses have been found in the spinal fluid of patients, and only a minority have had an antecedent illness associated with EV-D68. Case-control studies are planned to look for clues, but presently AFM is a mystery disease of unknown cause.
It is taboo to suggest a role for vaccines, but some old-timers remember “provocation poliomyelitis” or “provocation paralysis.” This is paralytic polio following intramuscular injections, typically with vaccines. PP was most convincingly documented by Austin Bradford Hill and J. Knowelden during the 1949 British polio epidemic when the risk of paralytic polio was increased 20-fold among children who had received the DPT injection (BMJ 2:1–July 1, 1950). Similar observations were made by Greenberg and colleagues in New York City; their literature review cited suspected cases as far back as 1921 (Am J Public Health 42:142–Feb.1952). I first became aware of PP 10 years ago while browsing through “Krugman’s Infectious Disease of Children” (page 128 of the 2004 edition).AFM may result from a direct virus attack on the spinal cord, or by an immune attack triggered by a virus, or by something else.
If a polio-like virus is circulating in the U.S., the possibility of its provocation by one or more vaccines has to be considered.
As Mawdsley writes in his Lancet article, concerns about polio provocation resurfaced in the 1980s, as vaccination programs increased in developing countries, and as a result, increasing numbers of children were being paralyzed. The United States has a history of doing the right thing when this happened in the 1950s. Unfortunately, that was before those entities in our government decided that protecting the children from harm was somewhere down on the list of priorities, well below protecting the program from “any doubts about the safety of the vaccine, whether or not well-founded…”
One final thought about Acute Flaccid Myelitis (AFM) before I close. According to the CDC, AFM is a biennial occurrence, with notable “outbreaks” happening every two years, beginning in 2014. There were increases in incidence in 2016 and in 2018. It was predicted that there would be a big increase in AFM in the late summer and fall of 2020, based on previous behavior of this particular “mysterious polio-like illness,” which affects children, and primarily those children who are at the age when they receive shots before going into kindergarten. However, in 2020, it didn’t happen. One might reasonably wonder if that could be the result of children not going to school and parents not taking them in for “routine, well-child appointments” where vaccines are given. We will never know, because it won’t be investigated. It can’t be. Because that would fall under the heading of “doubts about the safety” of vaccines, and we know that since 1984, those have not been allowed to exist.
Excellent summary. One more question. When was the polio "virus" even properly isolated, characterized and demonstrated to cause illness? Giving a vaccine during a time when paralysis is escalating would simply add more toxicity to the proven toxic causes of paralysis. Certainly isn't proof that the "live virus" caused anything
Wow, impressively researched and written. Thanks Marcella!