
Questions and Answers About Vaccinations
Do vaccines cause autism? Did vaccines save us from deadly childhood infections? What the research really shows...

This post is too long for email. Please click the button to view in the app.
The following is a presentation I put together a few years back. The information is still timely and relevant, as nothing has changed in the realm of the “safe and effective” mantra continuously repeated by CDC, FDA, ACIP, IOM, AMA, AAP, etc. They are still relying on the same studies, with the same issues reported in this presentation. They’ve just added more vaccines to the already ballooning schedule. There still hasn’t been a single study looking at the schedule as it is administered. And it is still true that when it comes to autism, the only vaccine they have looked at is the MMR, and the only ingredient is Thimerosal.
Many of the videos of me giving presentations have been removed from Facebook and from YouTube. There is (at this moment) a video of me giving a version of this presentation in 2014 when I was associated with the Cady Wellness Institute in Indiana. You can watch that video here and follow along with the slides in this post. The video will not marry up exactly with the slides because I have updated information where applicable.
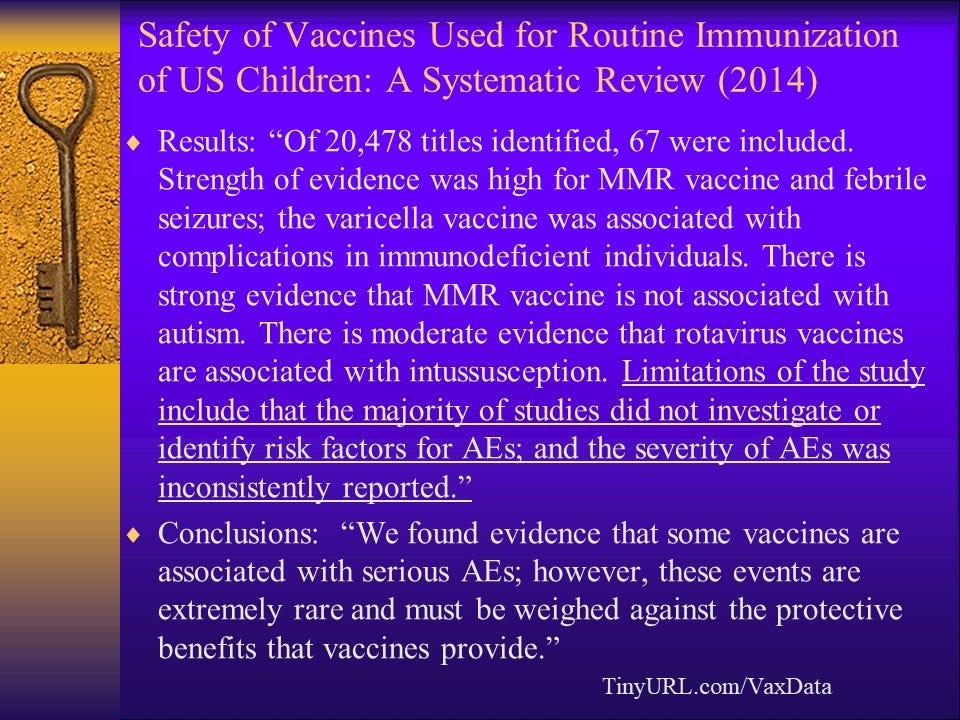
Here is the link for the study. My observation: of more than 20,000 studies, they included 67. That does not sound “systematic” or comprehensive in any way to me, so I looked up the definition of “systematic.” The definition of systematic: Done or acting according to a fixed plan or system; methodical. Example: “A systematic search of the whole city.” That is confusing. Looking at 67 studies out of a body of 20,478 certainly doesn’t sound like they searched “the whole city.” However, considering the way that vaccine research is routinely done, it is entirely conceivable that they went into this endeavor with a “fixed plan” in place. Altering study protocols to find what “needs to be found” is not an anomaly among researchers seeking to absolve vaccines of the harm they do.
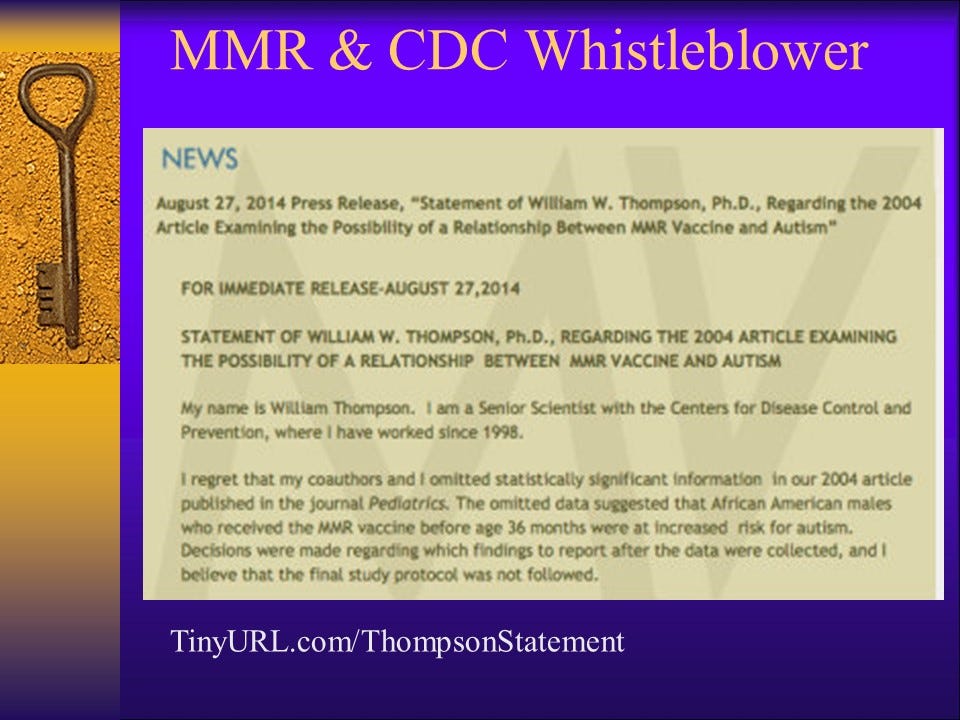
Dr. William Thompson’s press release has been removed from the website of his attorneys. You can find the complete statement here.
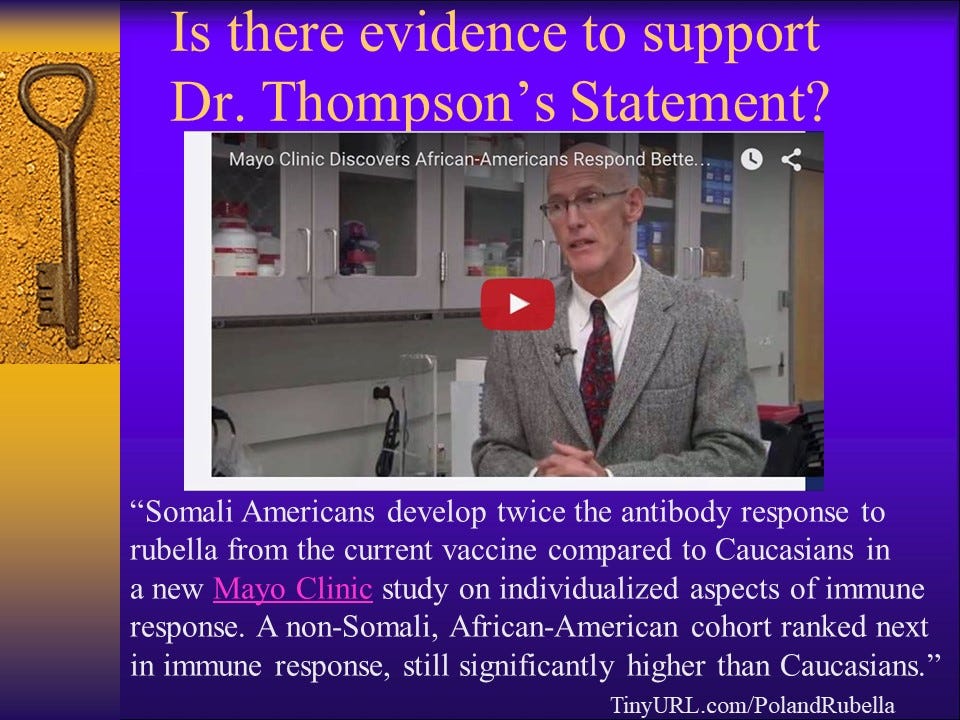
… potential risk from over-vaccination. That’s an important (and RARE) admission.
As noted above, the MMR vaccine is the ONLY vaccine that has ever been researched (by the government-sanctioned agencies) for its effect on the increasing incidence of autism. Of the MANY ingredients in vaccines, Thimerosal (which is approximately 50% mercury) is the ONLY ingredient that has been studied with regard to autism. Most of that research was conducted by Poul Thorsen.
Poul Thorsen is still wanted by the FBI and the CDC is still relying on his research for their conclusion that “Thimerosal does not cause autism.”
Click here to watch a video clip from Dr. Healy’s interview with Sharyl Attkisson at CBS News.
Click here to read more of Dr. Healy’s interview with Sharyl Attkisson.
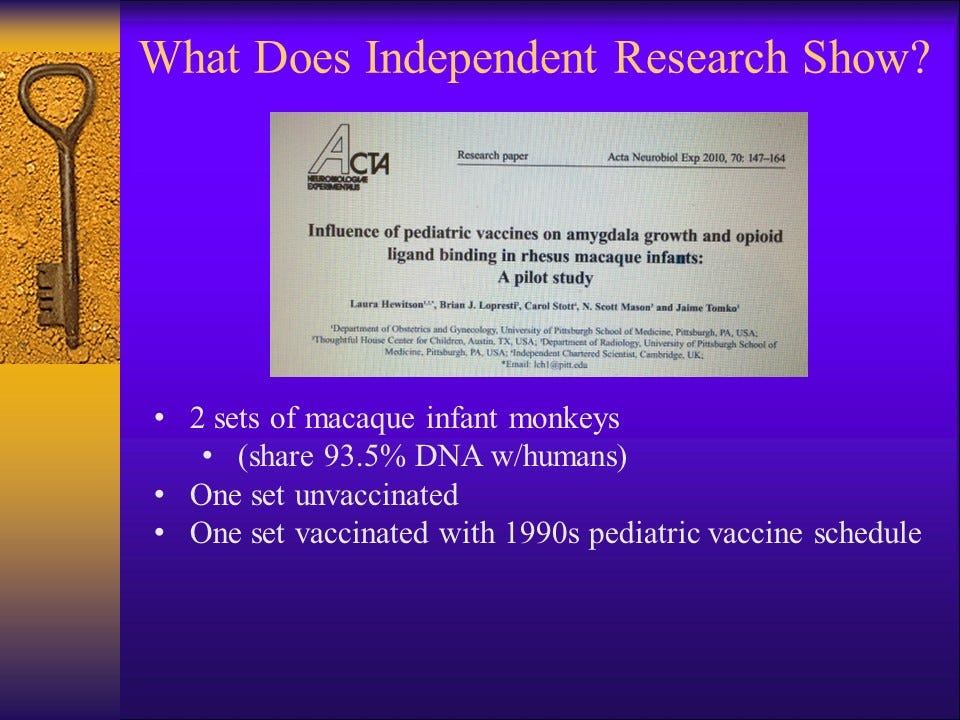
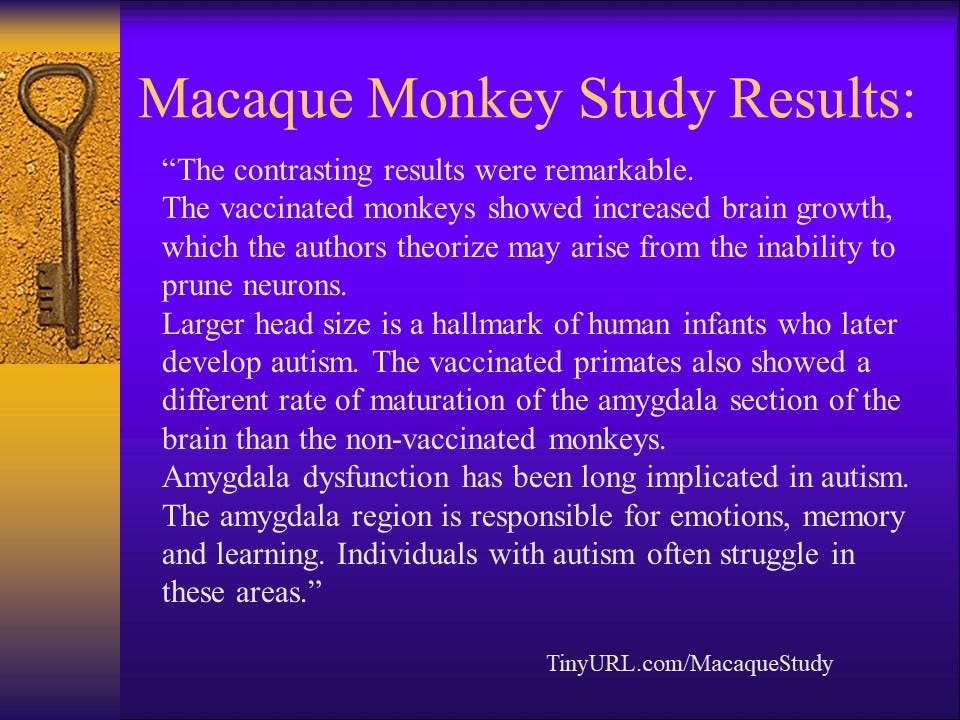
And, the follow-up study…
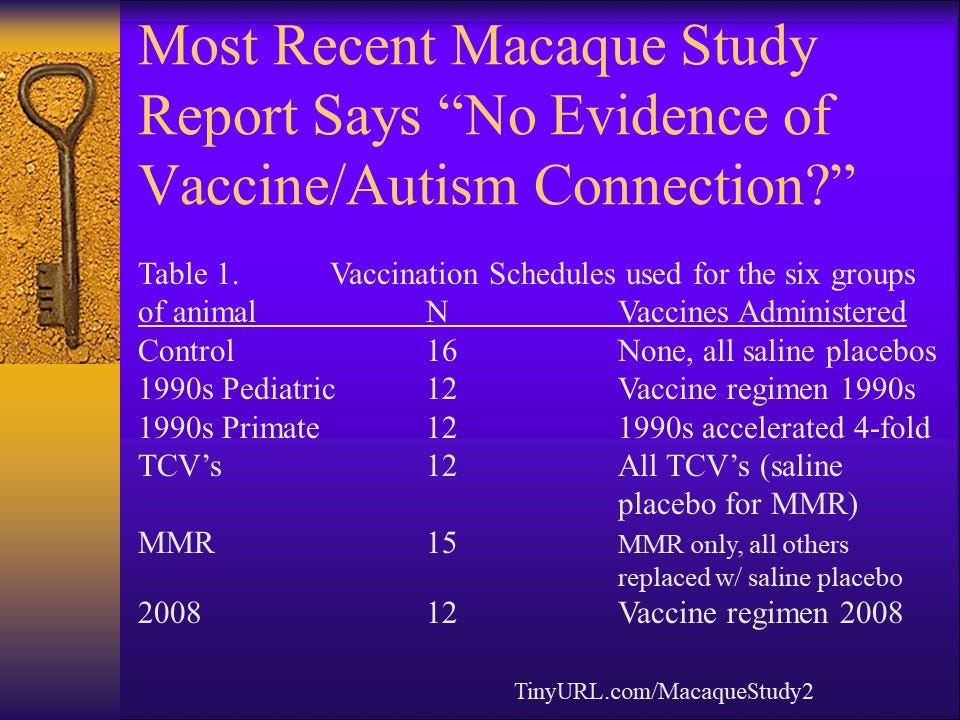
There are some big problems with this study. The first thing that is glaringly evident is that the study groups are extremely small. At the time the study was conducted, the official rate of autism (per the CDC) was 1 in 68 American children. In order for the results to be valid and generalizable to the population of human children, there would have to be at least 68 macaques in each study group. I wrote a critique of this study in 2015 and published it on VaxTruth. You can find it here, via the Wayback Machine.
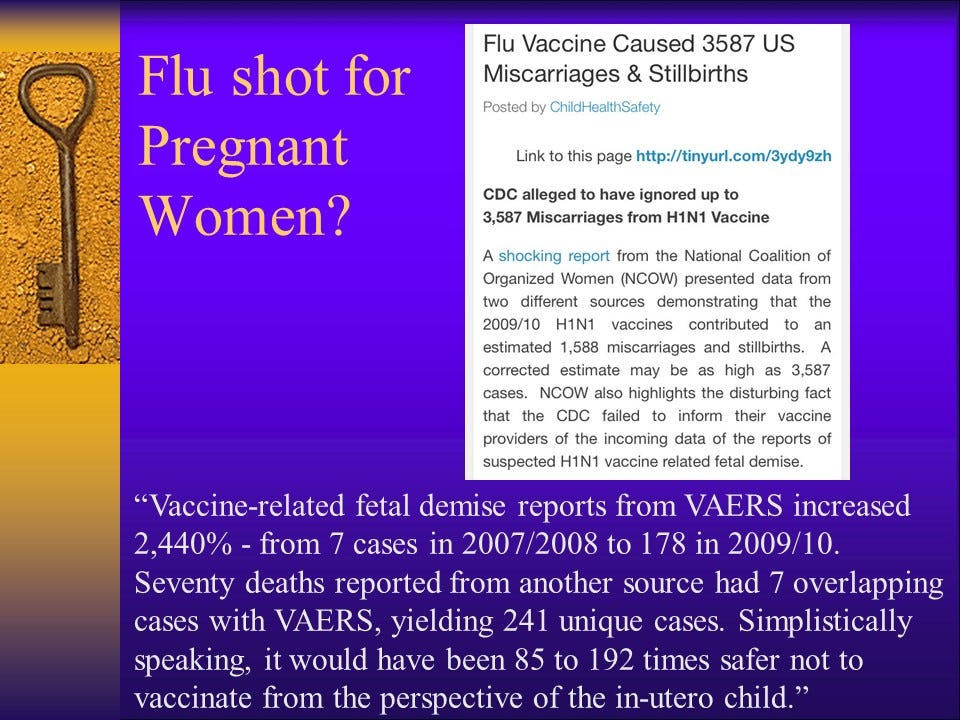
As previously noted, the bulk of “vaccine safety research” conducted by the CDC has focused on either the MMR vaccine or Thimerosal. You may have heard that Thimerosal (mercury) has been removed from childhood vaccinations. This is not true. While it is true that there is far less mercury in childhood vaccinations than there was during the 1990s, Thimerosal is still being used in the manufacturing process of many childhood vaccines and is present in “trace amounts.” The FDA has altered the rules and allows manufacturers to continue using Thimerosal without having to declare it on the label, as long as Thimerosal is not being used as a preservative. And then there is the issue of multi-dose flu shots given to pregnant women and children. Each adult multi-dose flu shot, including those given to pregnant women, contains 50 micrograms of Thimerosal, which is 25 micrograms of mercury. The children’s multi-dose flu shot contains half the amount at 25 mcg Thimerosal (12.5 mc. mercury).
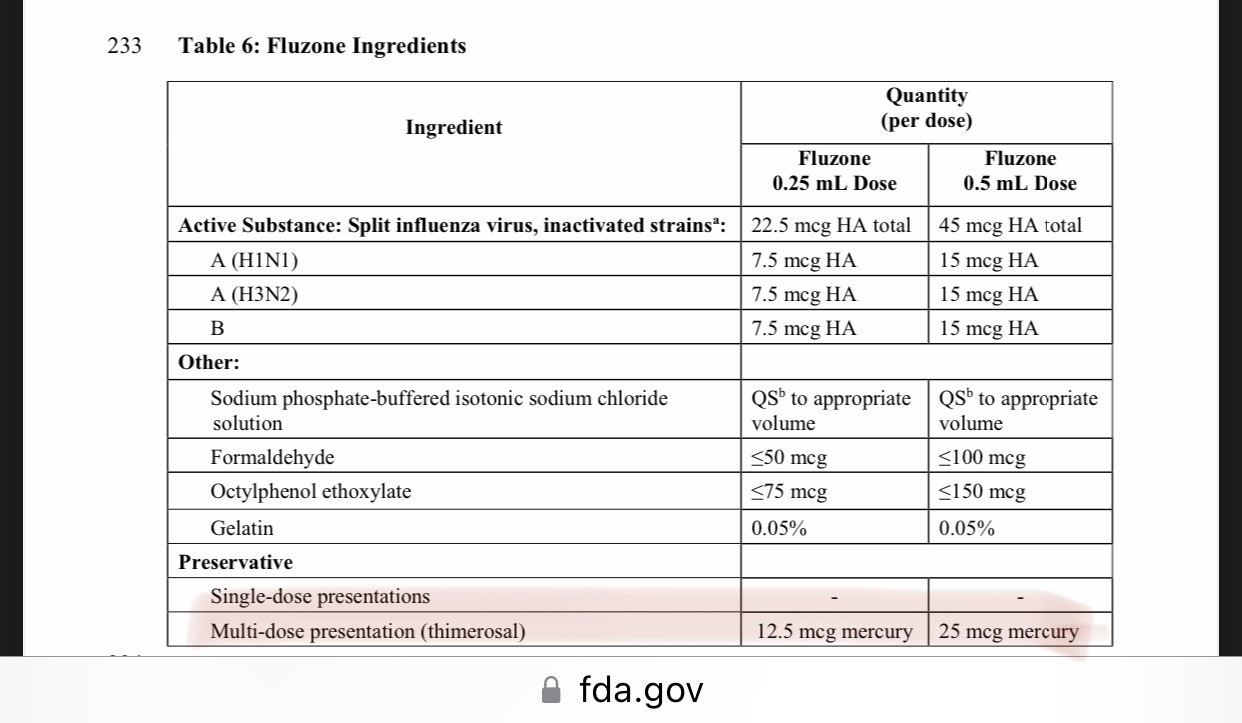
Link for the FluZone manufacturer’s insert. Here is where you can find other vaccine manufacturer’s inserts for vaccines licensed in the United States.
As mercury was being “removed” from childhood vaccinations, the amount of aluminum used as an adjuvant (to stimulate the immune response) was going up. The “official word” on aluminum (from the CDC and the likes of Paul Offit) is that aluminum is safe when injected because “there’s more aluminum in breast milk than there is in vaccines.” As I have noted time and again, if America’s “best and brightest” scientists at the CDC don’t know there is a big difference between ingestion and injection, when it comes to drug (and toxin) delivery and effects, we have more problems than we ever dreamed of.
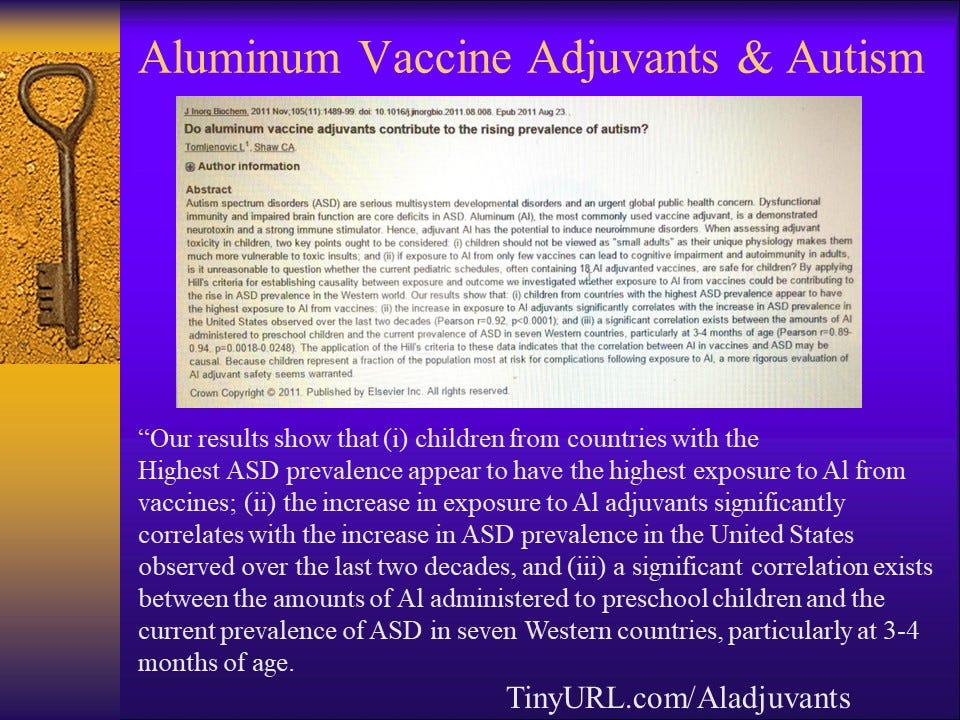
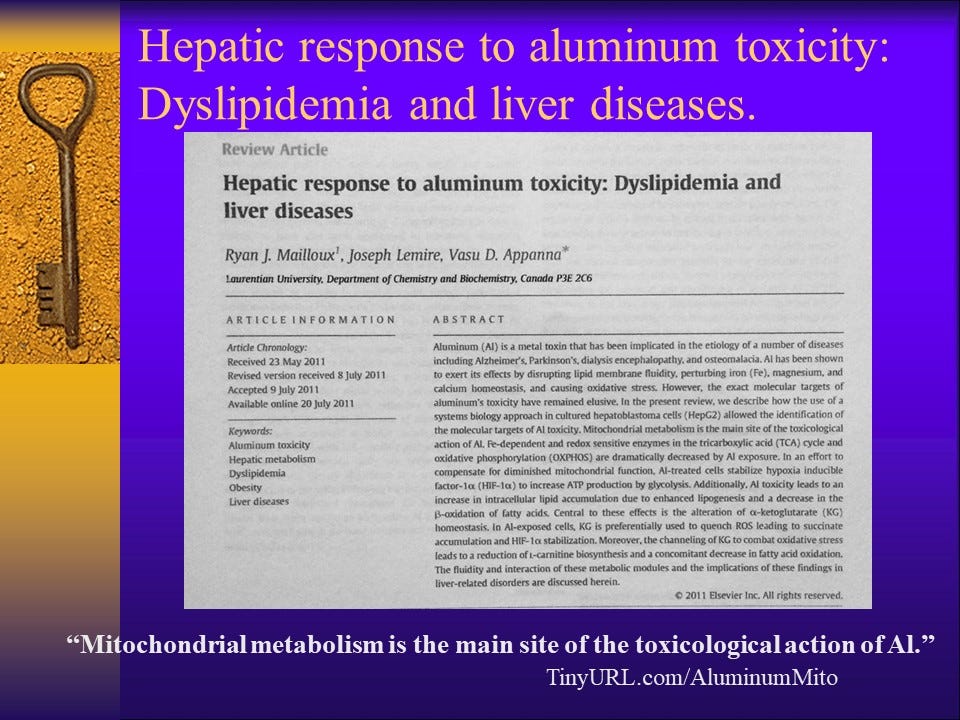
Link to the study. Here is what the CDC has to say about mitochondrial disorder and autism. Of course, they have no idea what may be causing either of these conditions, or why they tend to occur in children after vaccinations. They also say there are no studies… Which, of course is a lie.
On October 20, 2015 I attended a talk at the University of Southern Indiana. Dr. Andrew Kroger, the CDC’s Vaccine Education expert was speaking to students in the pre-med and nursing programs. His presentation focused on four main ideas:
Vaccines are the most miraculous invention in modern medicine.
Vaccines save millions of lives every year.
The CDC Childhood Schedule is the ONLY vaccine schedule. Do not deviate.
When parents ask questions, assert your authority. Belittle, shame, and threaten to leave them without medical care, if necessary. Stick to the schedule.
I audio-taped the entire presentation and shared it to my YouTube channel. It has been removed for “violating YouTube’s Community Guidelines.” To be clear, the entire content of the video that was removed was the audio of Dr. Kroger’s presentation and the questions asked (and his answers) at the end of that presentation. So now, we are not even allowed to know what the CDC’s Vaccine Education Expert is telling future doctors and nurses?
This is the detail I wrote about the video when I posted it on October 20, 2015:
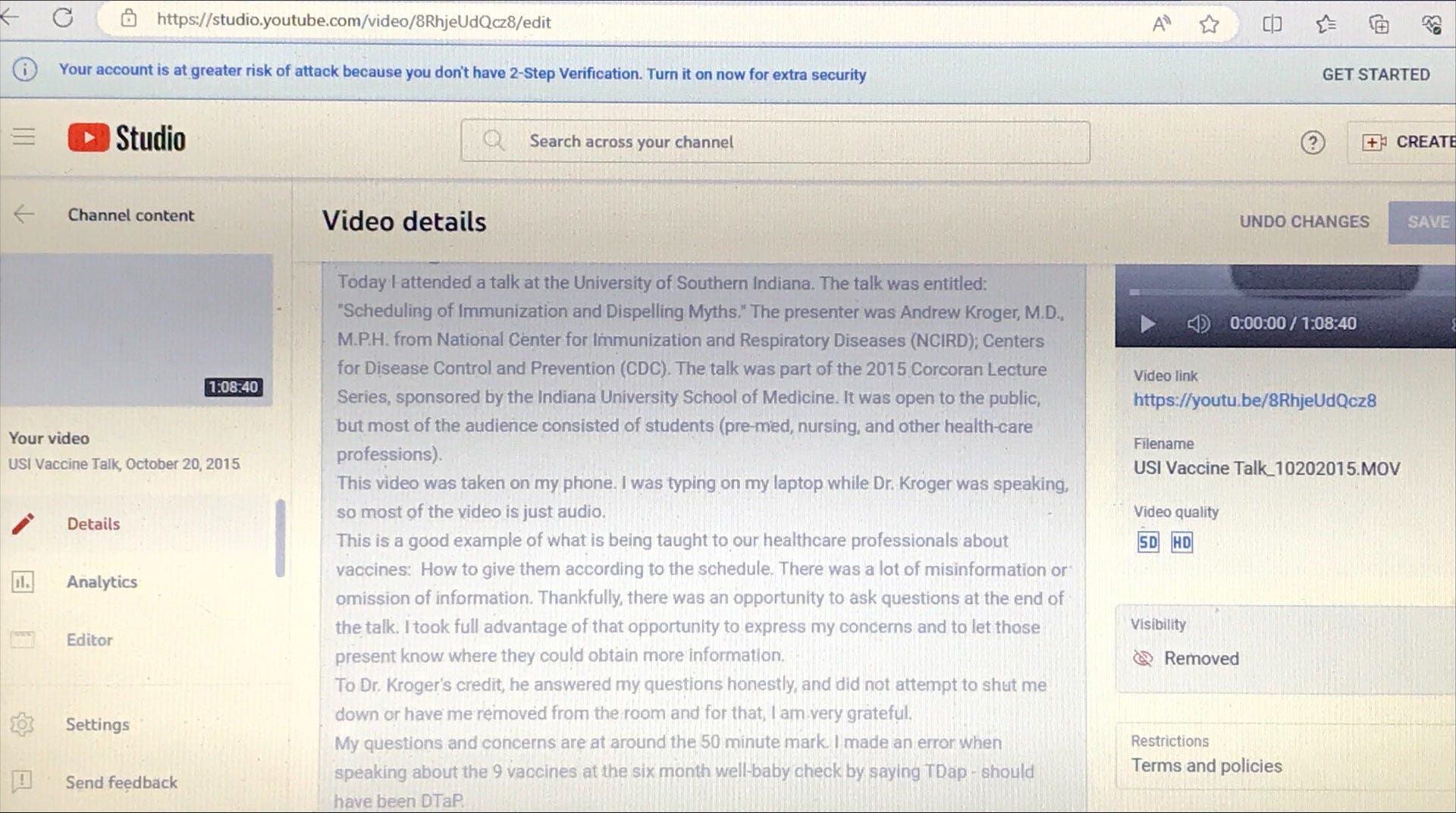
One of the issues I raised at the end of Dr. Kroger’s presentation was the fact that the CDC’s Childhood Schedule has never been studied. I stated, “There has never been a single study to investigate the effect of vaccines as they are administered.” Dr. Kroger’s response? “You are correct.”
He went on to state that the reason this has not been done is because “there are so many vaccines now” and “it would be unethical” to study the effect of those vaccines as they are administered because doing so would leave some children (the control group) unvaccinated and therefore “unprotected.”
You can listen to the exchange in this short video.
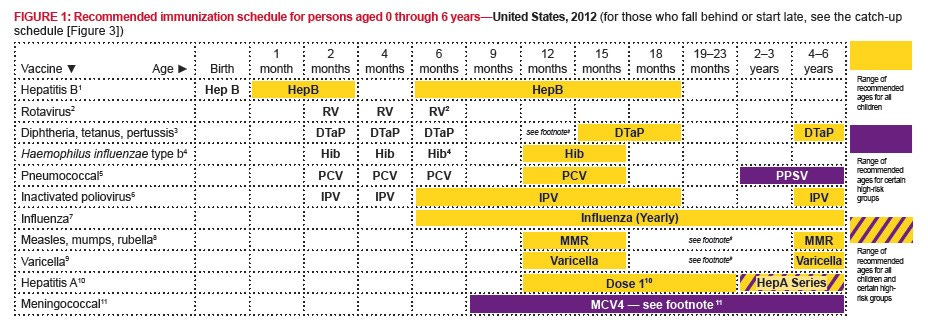
At the time when I first put this information together, The United States was still using the 2012 CDC Childhood Vaccine Schedule. Here is what that looked like for children birth through age 6 years:
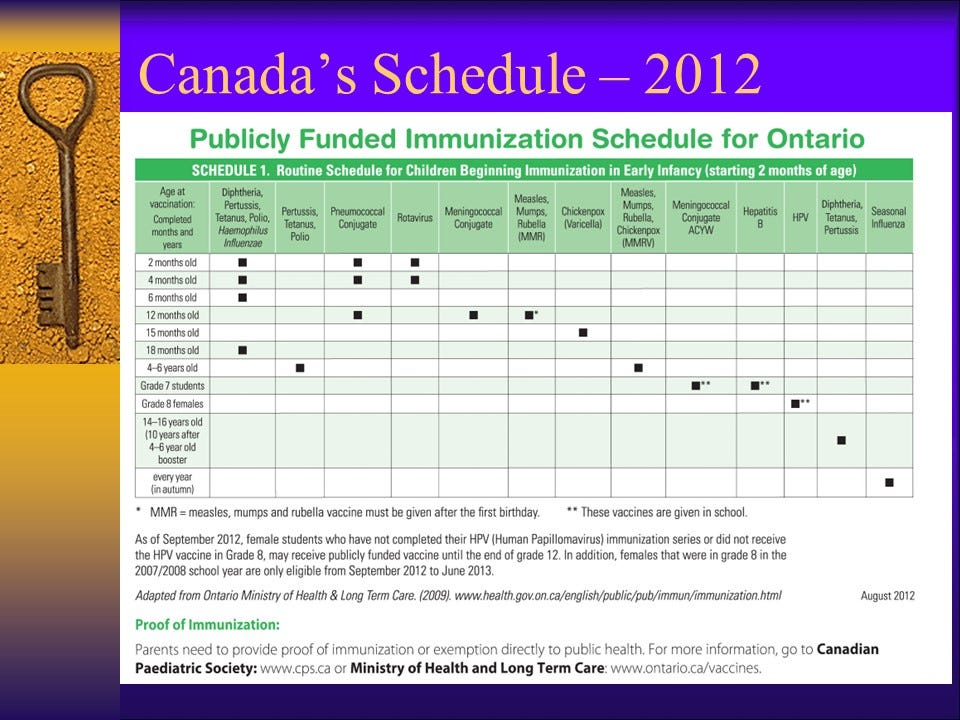
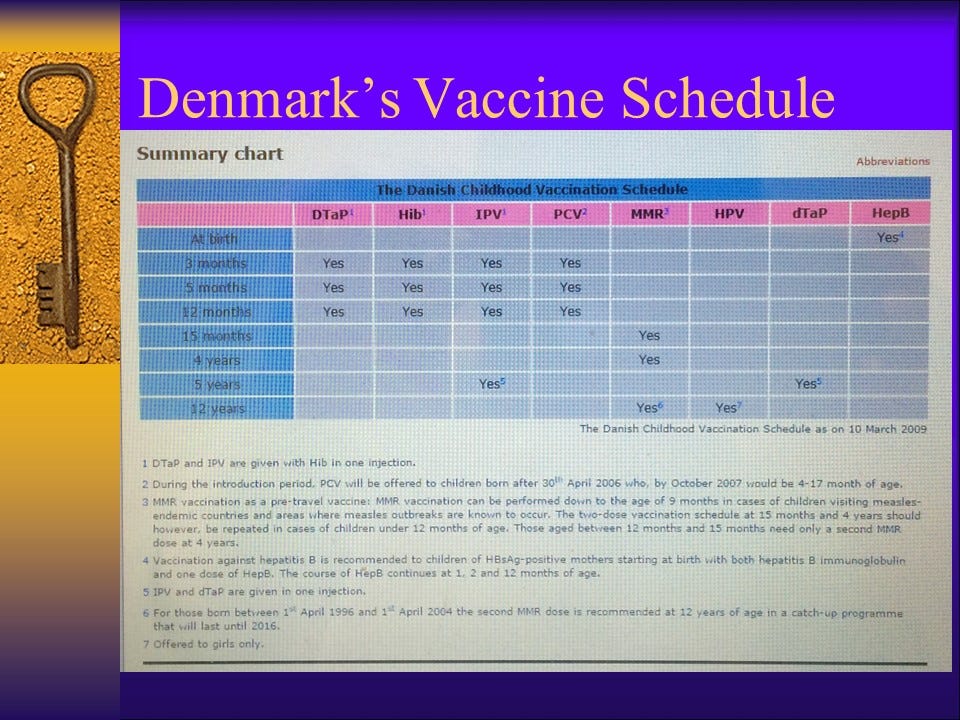
And for comparison:
Have you heard about the United States’ abysmal Infant Mortality Rate (IMR)? Here is the link from 2010, referenced in this presentation. If you’ve been paying attention, you may have heard that the U.S. Infant Mortality Rate continues to go up, with a significant increase in the last three years (since 2021).
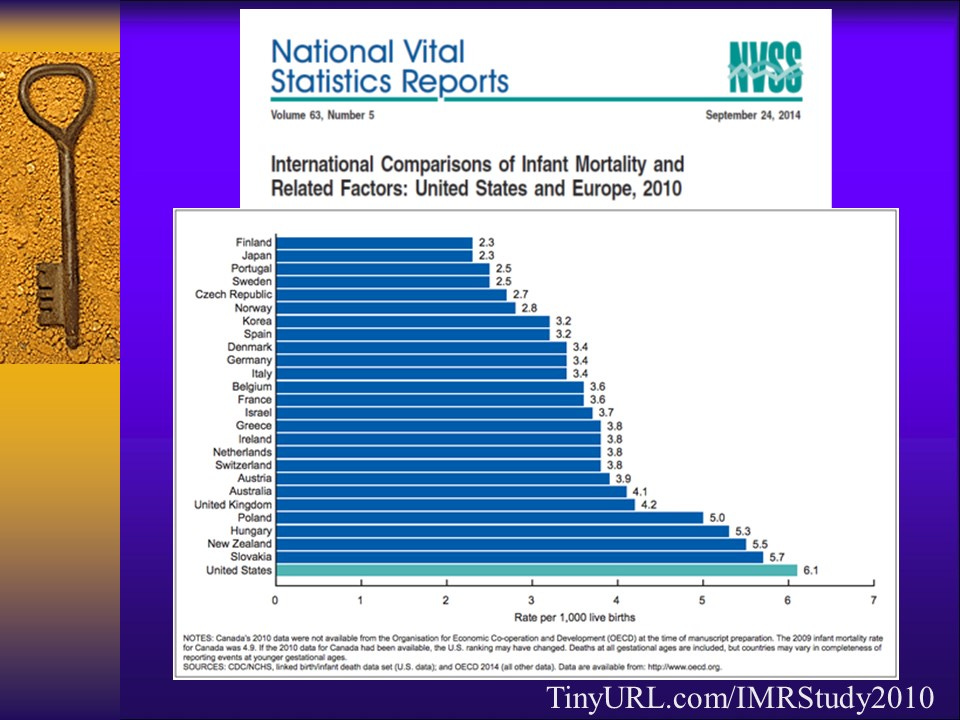
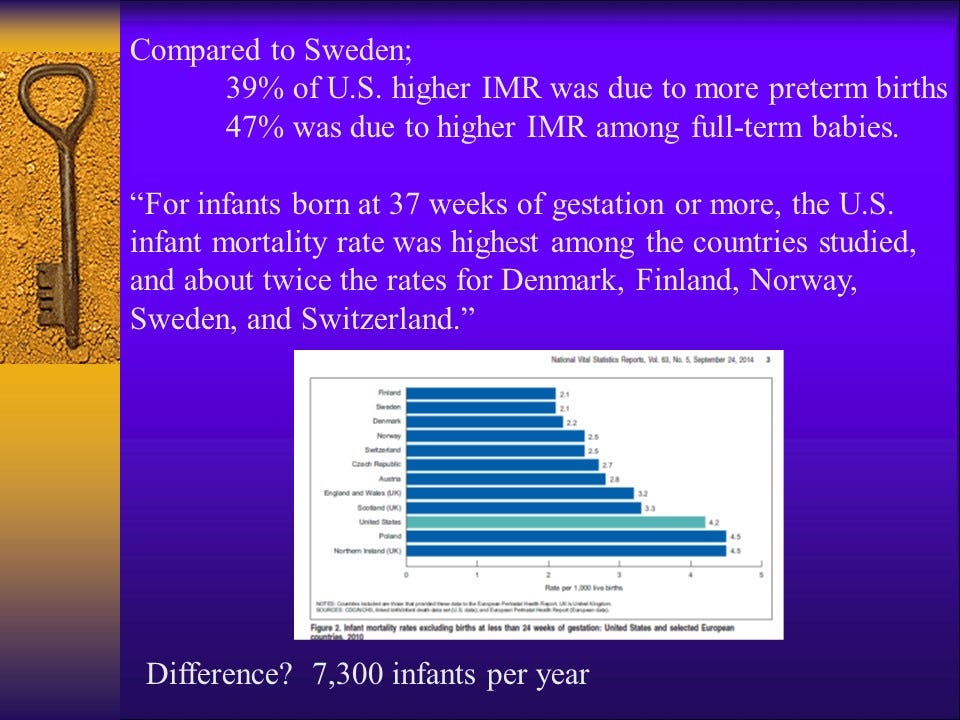
In 2010, The United States ranked 26th among developed nations, with an Infant Mortality Rate that was nearly three times the rates of Finland, Japan, Portugal, and Sweden (the four countries with the best IMR). One of the things that is often repeated when it comes to the IMR is that the United States has a higher rate because we go to extremes to save babies who are born extremely early and at extremely low birth weights. The 2010 report looked further into this and found that even when the effect of pre-term births was factored out, the U.S. had the highest IMR rate among developed nations. Among American infants born at full-term (37 weeks and beyond), nearly double the number of babies were dying before their first birthdays when compared to other nations with similar socio-economic status.
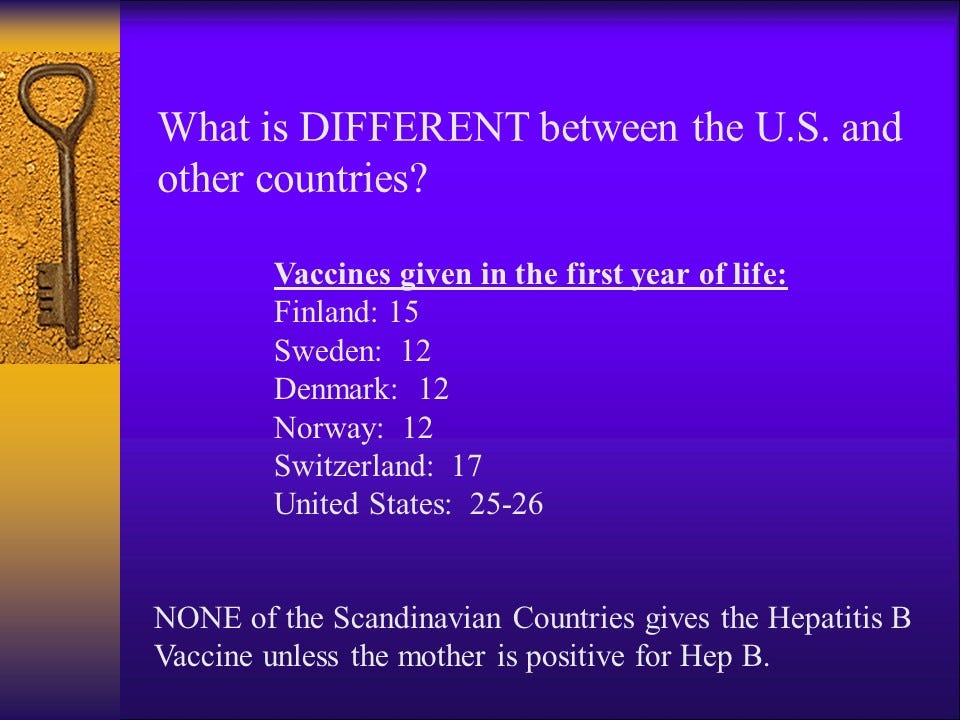
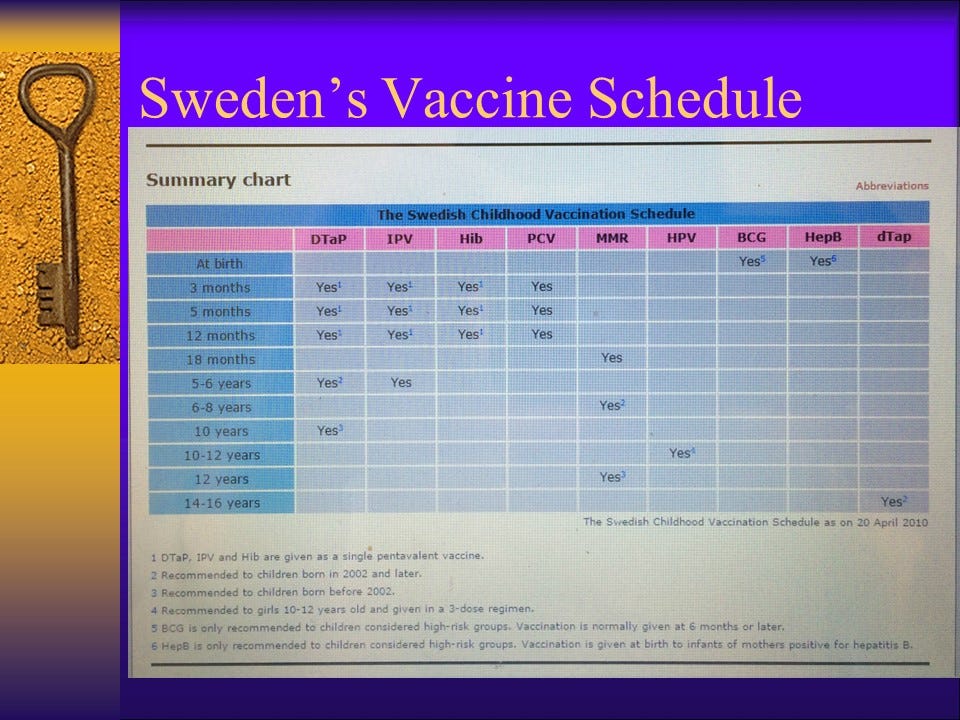
Note: This presentation was developed in 2014. Other countries have begun to administer the Hepatitis B vaccine on a routine basis, and the effects of this need to be studied to see what, if any changes to the IMR correlate.
The United States’ Childhood vaccine schedule exploded after the 1986 Law granted manufacturers freedom from liability when their vaccines injure or kill.
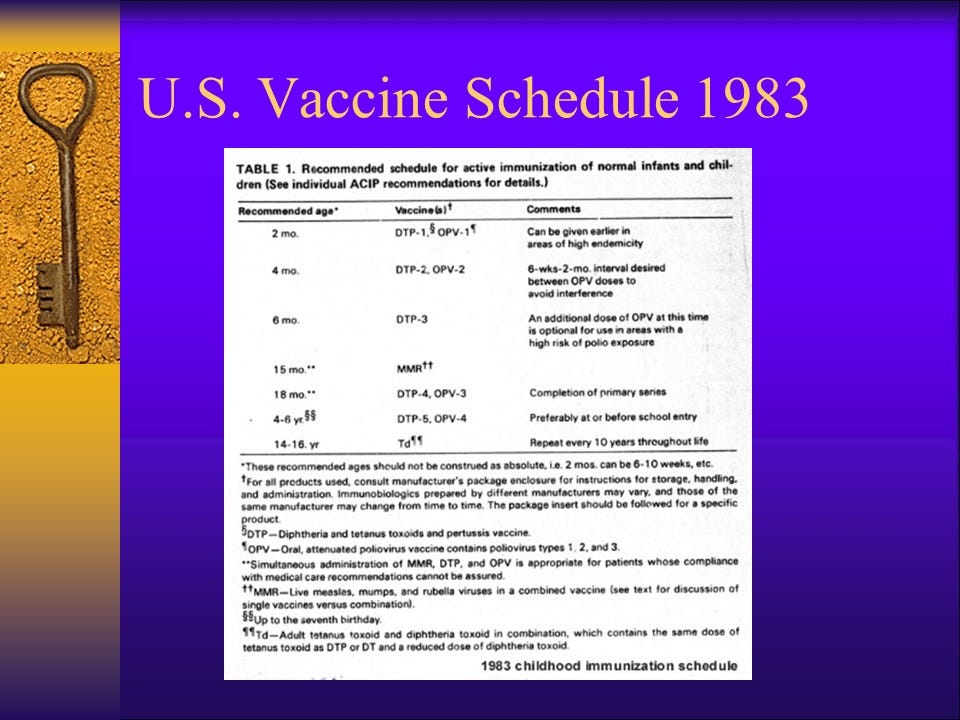
The above slide shows the United States Childhood Vaccination Schedule from 1983.
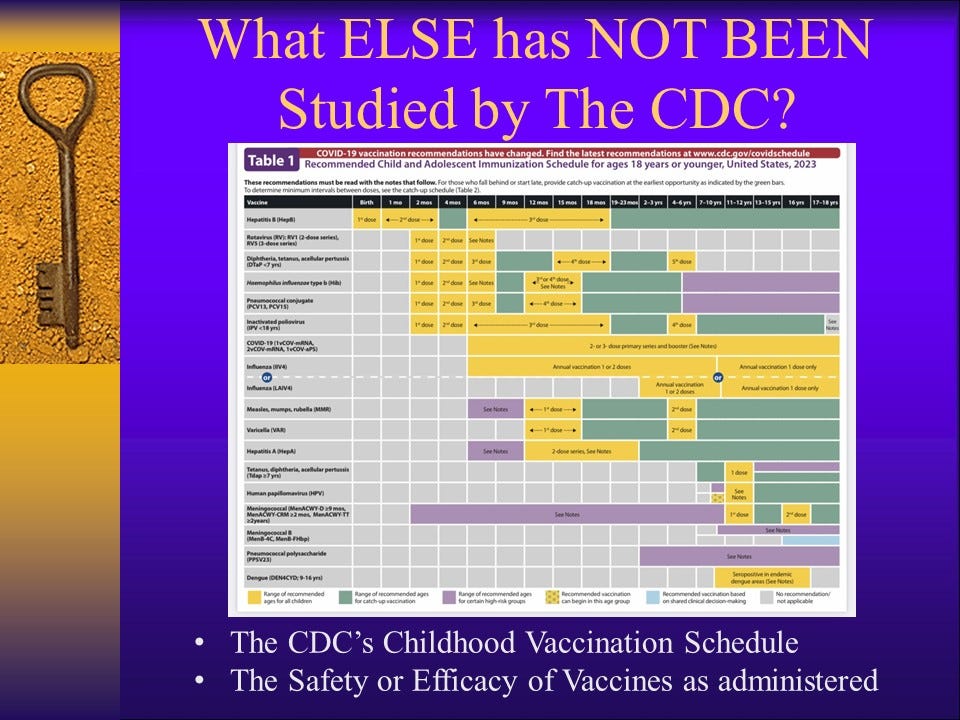
The next slide shows the United States Childhood Vaccination Schedule for 2023. Just as an aside, in the 1980s, the rate of autism in the United States was estimated at 1 in 10,000 children. The 2023 CDC estimate on the prevalence of autism is 1 in 36 American Children. The incidence has been increasing at a rate of 13% per year since at least 2000. The CDC studies the prevalence rates every two years, and their survey is done on 8-year-old children. It takes them four years to report their data. The “current” estimate does not include any children under the age of twelve. It’s a VAST underestimate.
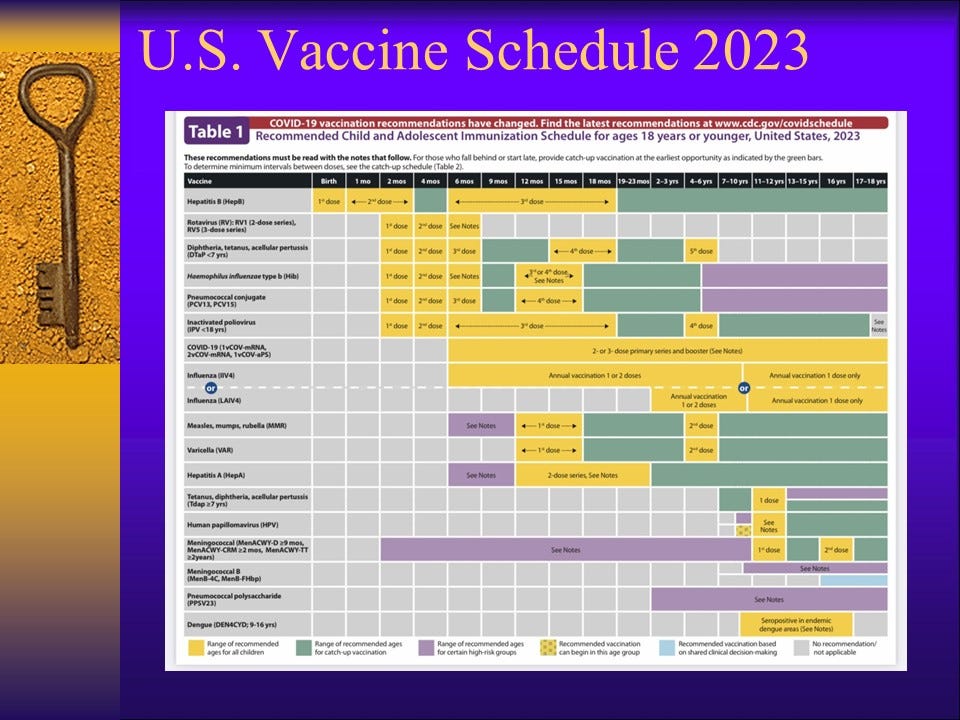
The CDC Childhood Schedule has more than quadrupled since autism rates were 1 in 10,000. The CDC has not studied the effects of this, and they won’t study the effects of this because, “That would be unethical.”
Let’s look at a few of the individual vaccines, which have NOT been studied by the CDC, starting with the Hepatitis B vaccine, which is given to American infants within 12 hours of birth, and 2-3 times more by age six months of age.
(Source)
The last time I updated this presentation this was what I found in VAERS:
Today’s query yielded the following results.
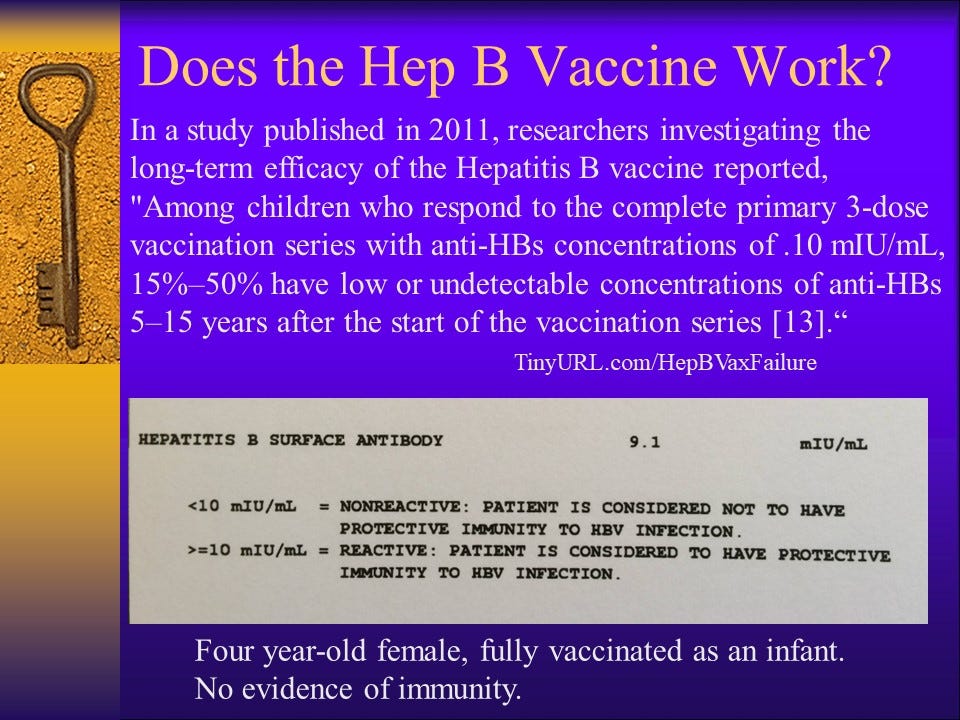
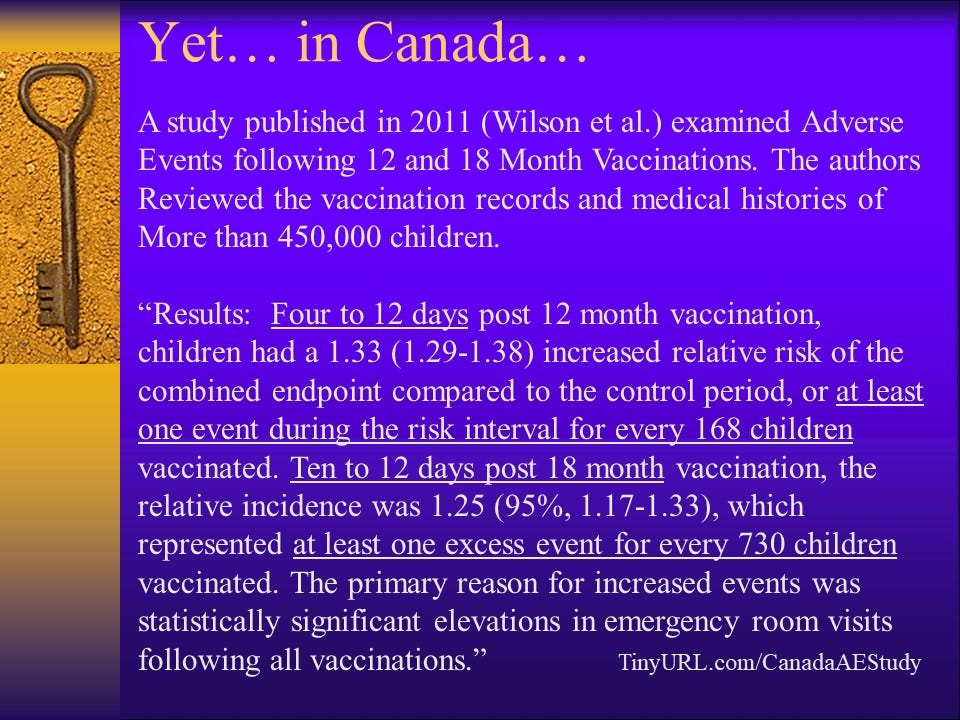
Note: The 2011 study referenced above can no longer be found on the internet. The waning immunity from Hepatitis B vaccination in infancy is referenced in this article (citation number 4). Let’s think about this for a moment. Up to 50% of infants who receive the Hepatitis B vaccine series between birth and six months of age have no evidence of protection from hepatitis B by the time they are 5-15 years old. Hepatitis B is primarily spread through sexual contact or sharing needles. This is clearly a case of all risk and no benefit for the vast majority of children who receive this vaccine as infants.
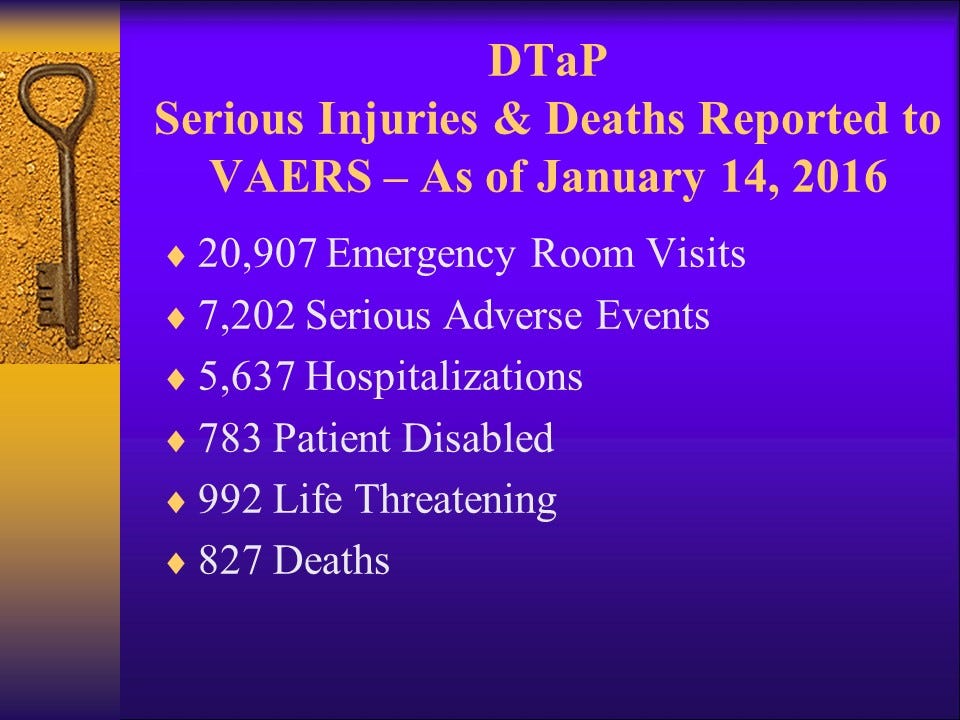
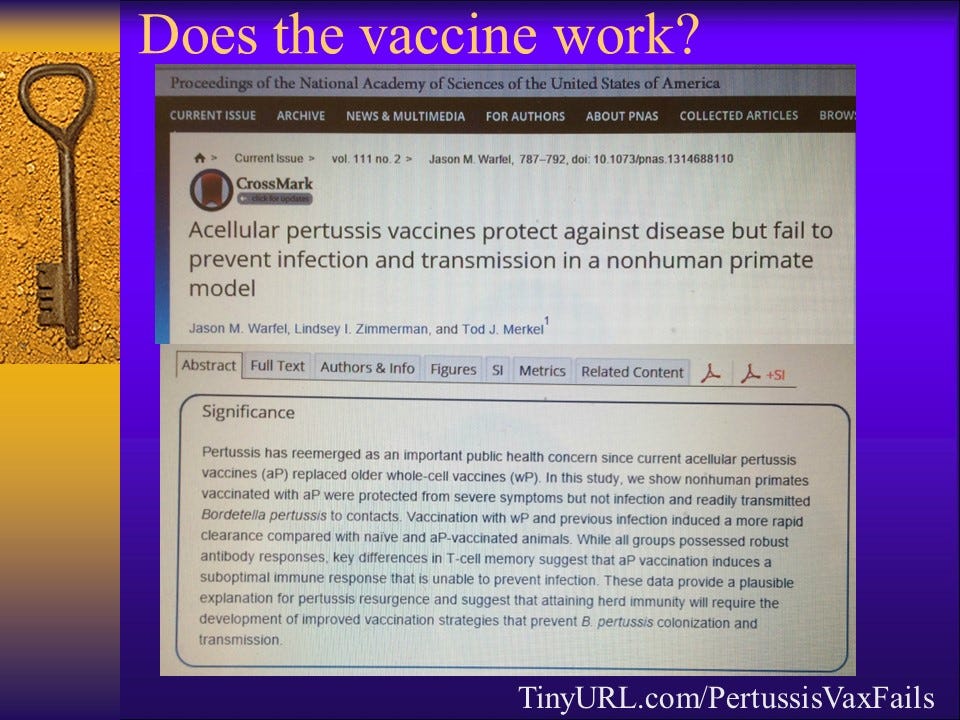
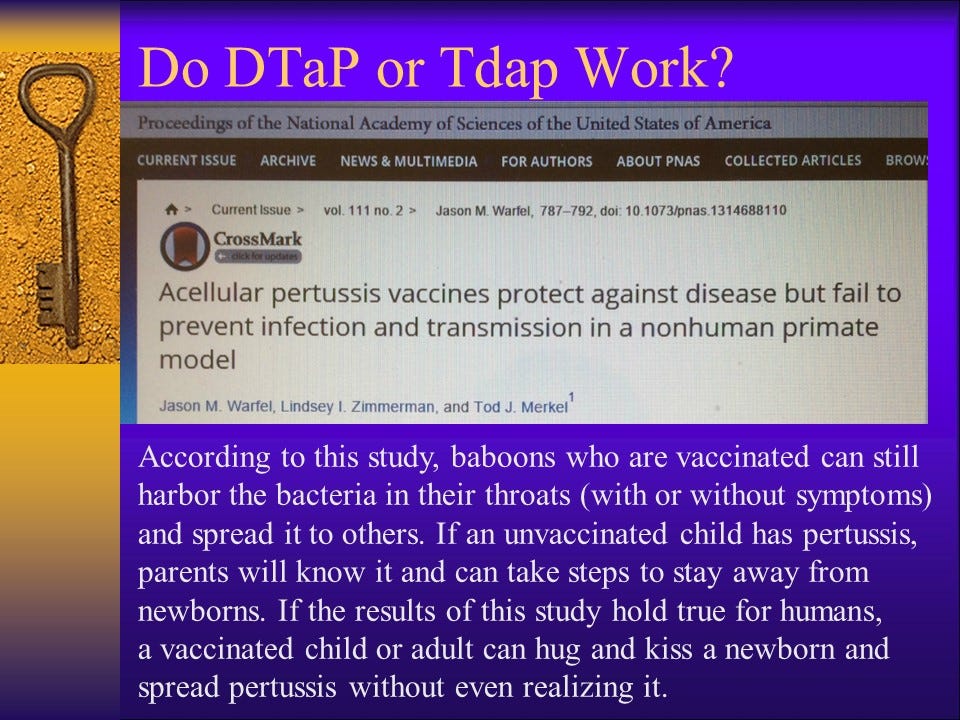
What about DTaP?
The last time I edited this presentation, these were the numbers for serious adverse events in VAERS from DTaP and DTaP containing combination vaccines like Pentacel and Pediarix, both of which have become quite popular with doctors because they can give five vaccines with one jab, giving parents a false sense of security, thinking their tiny infants are not really receiving all of those vaccines simultaneously.
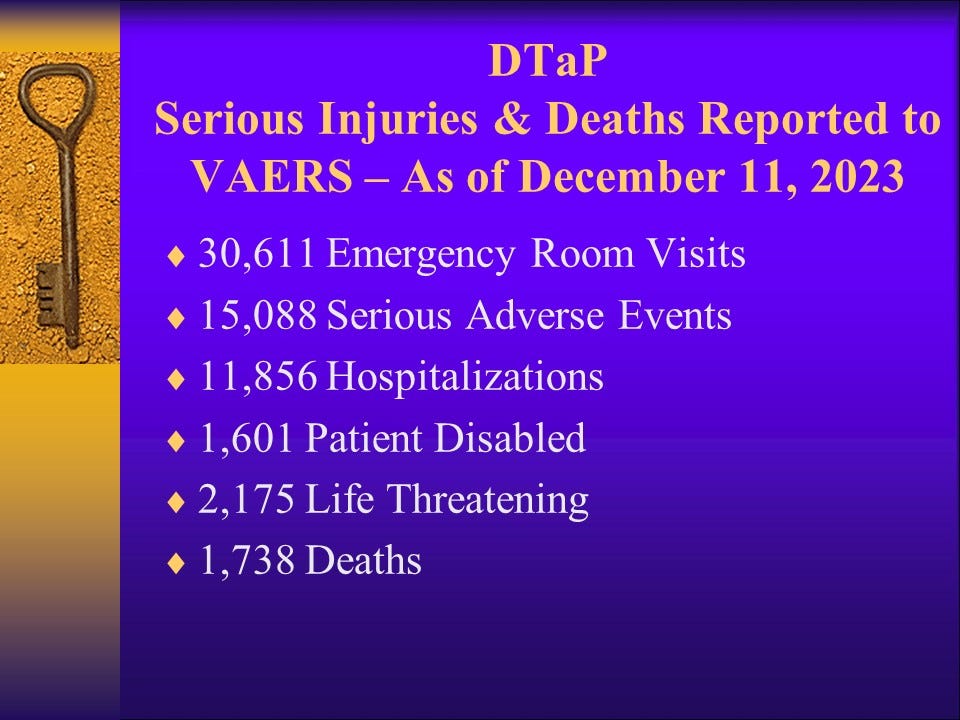
The same queries performed today (December 11, 2023) returned the following results.
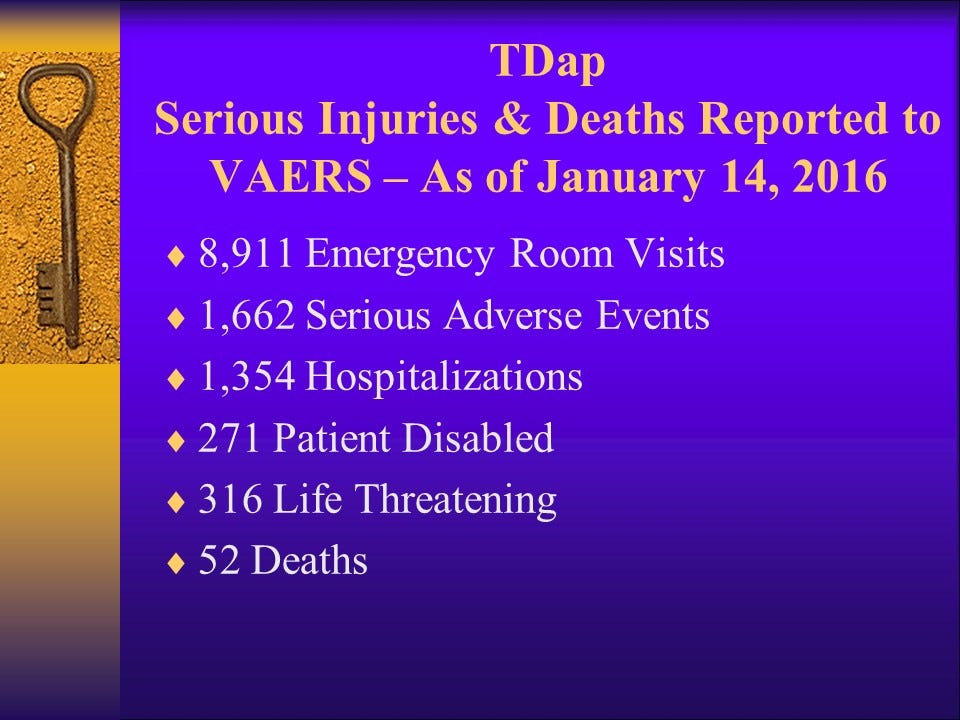
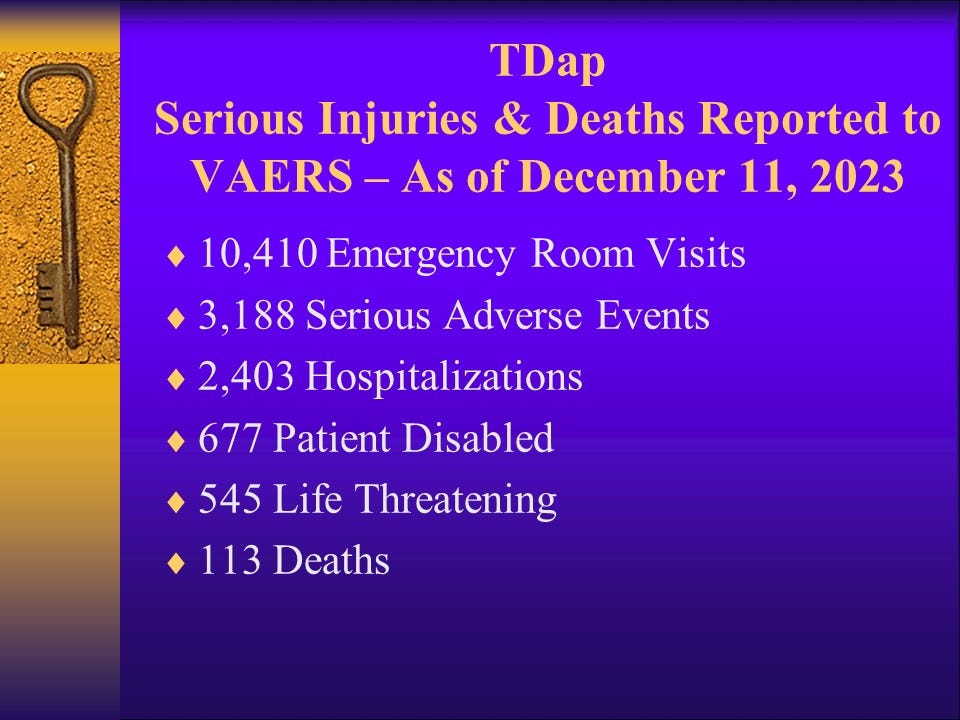
DTaP and DTaP-containing pentavalent vaccines are given to infants and children up to seven years of age. After the age of seven, a child is given the TDap vaccine. Here are the VAERS numbers for TDap:
The same queries today (December 11, 2023) returned the following VAERS numbers for TDap.
(Source)
(Source)
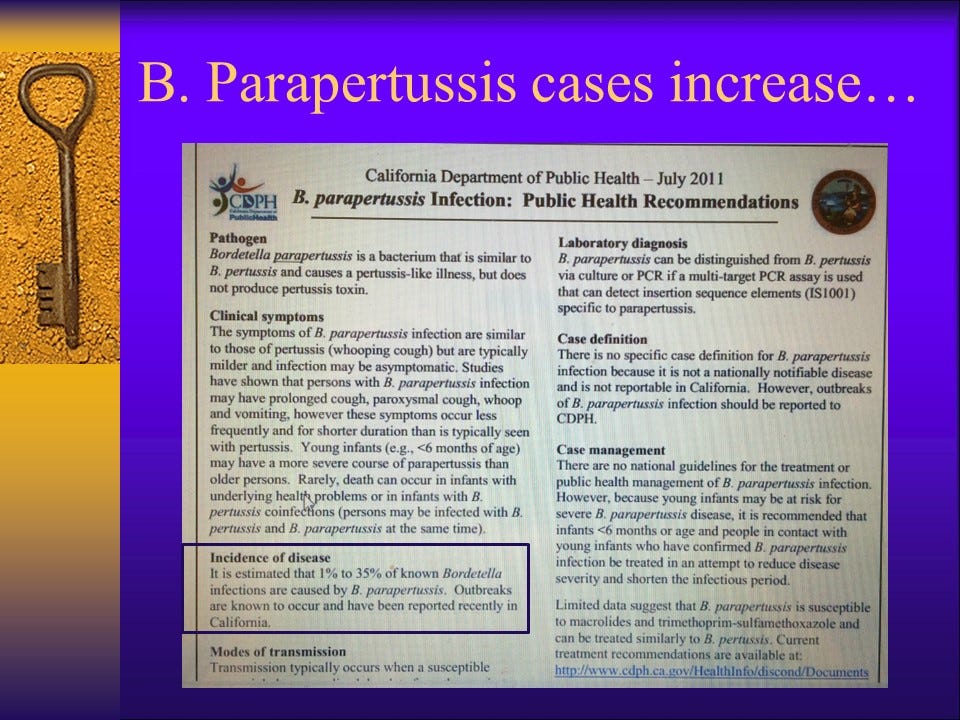
(Source)
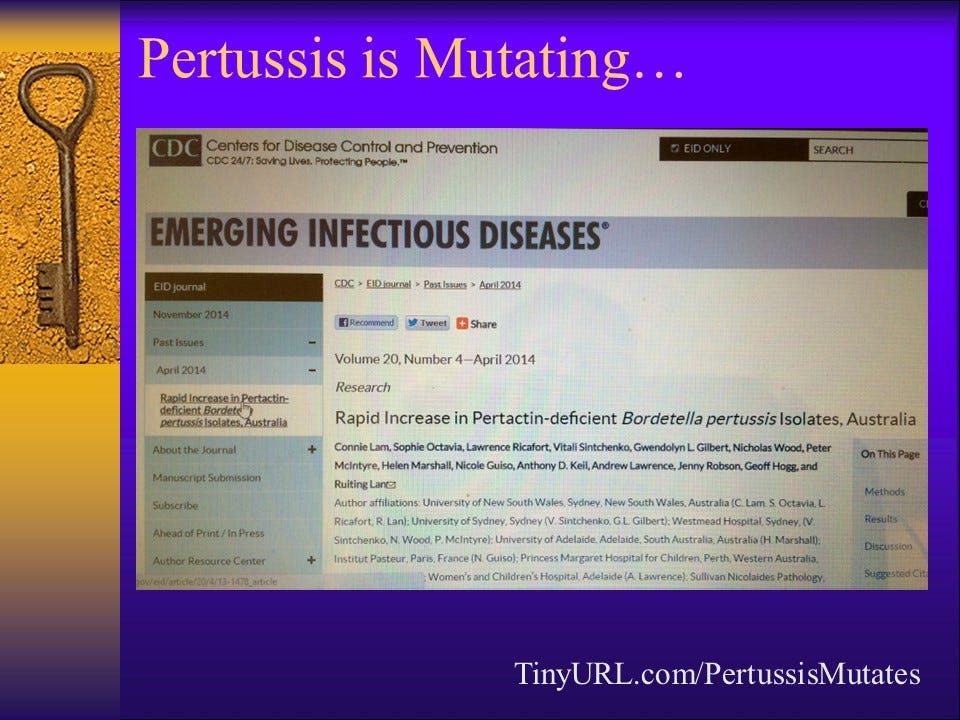
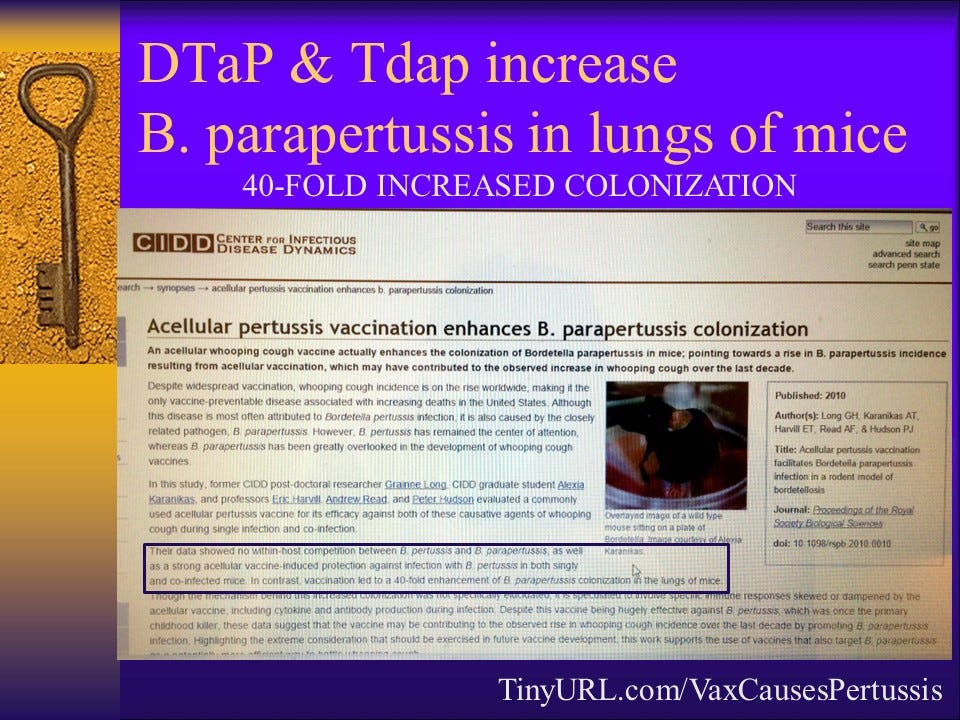
So, the vaccines (DTaP and TDap) that are supposed to protect against whooping cough are actually increasing the spread by promoting enhanced colonization of B. Parapertussis in vaccinated people, who are made 40 TIMES more likely to become infected and to transmit parapertussis if exposed than they would be if they had not been vaccinated. Even in the absence of symptoms. That is terrifying when it comes to the practice of “cocooning,” where entire families (parents, grandparents, siblings) are being told to “get the TDap to protect the baby.”
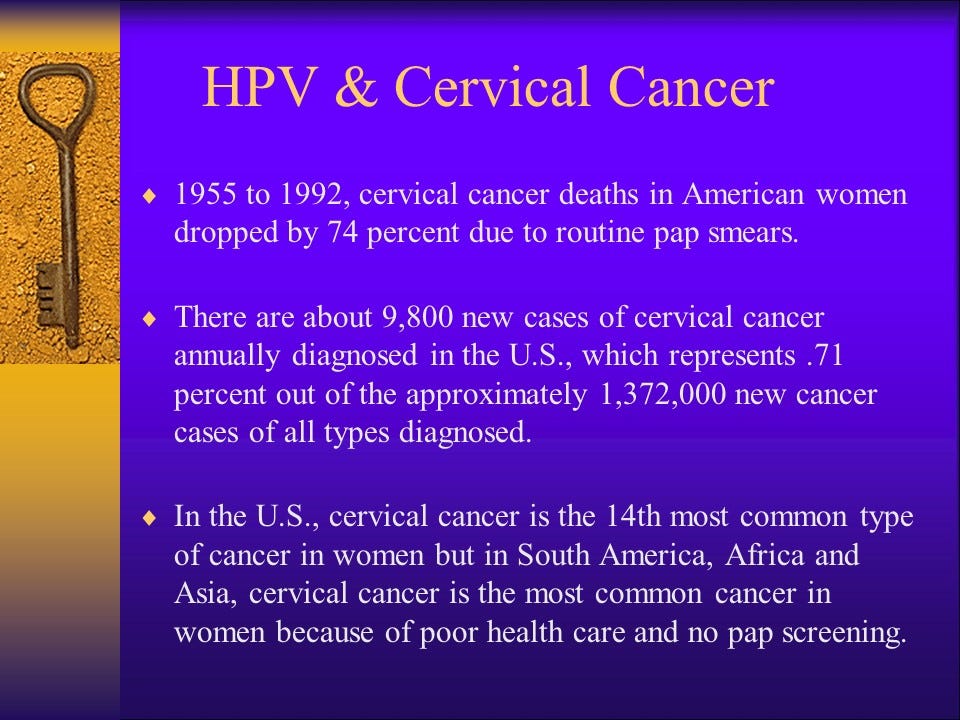
Let’s talk about HPV and Gardasil.
Note: The following slides were originally prepared in 2014. I have a more recently updated and expanded presentation about HPV and Gardasil, which I hope you will check out and share. You can find that here.
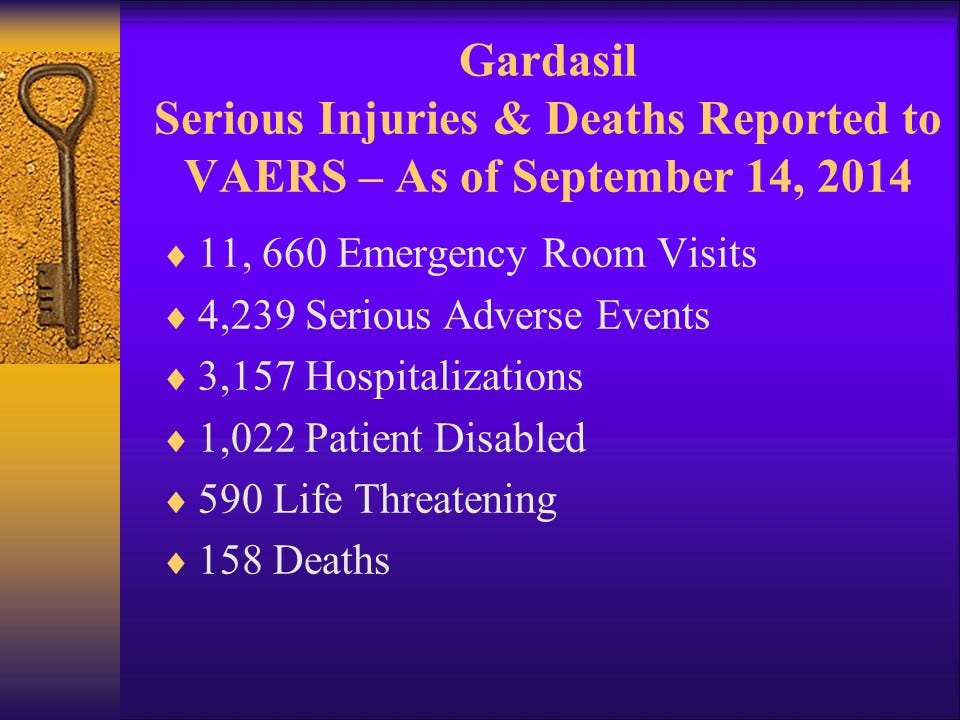
VAERS data from 2014:
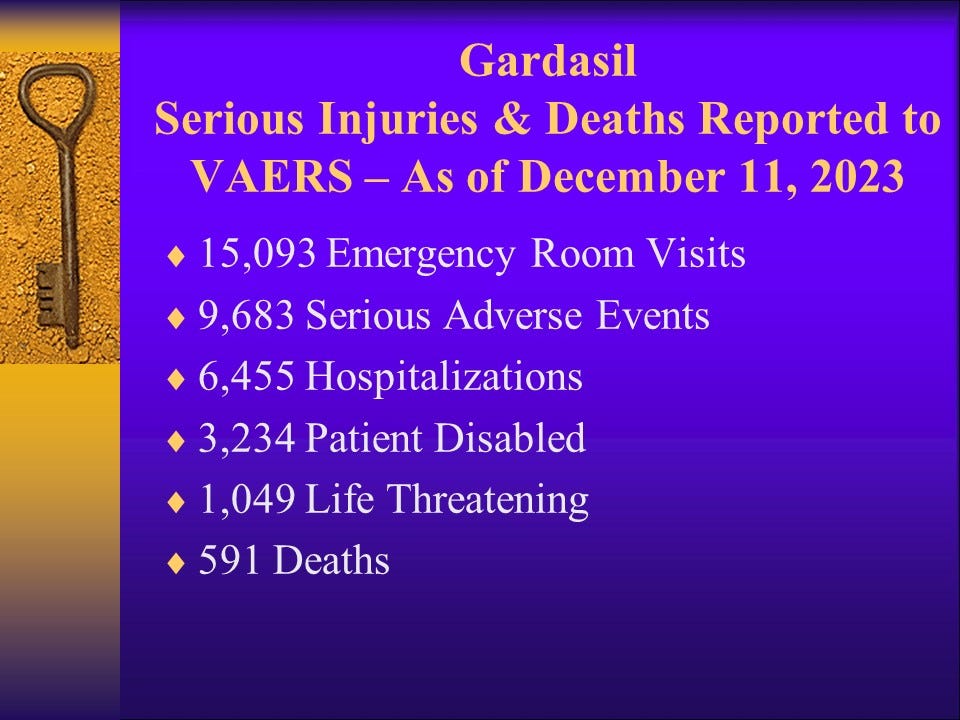
VAERS data from today (December 11, 2023):
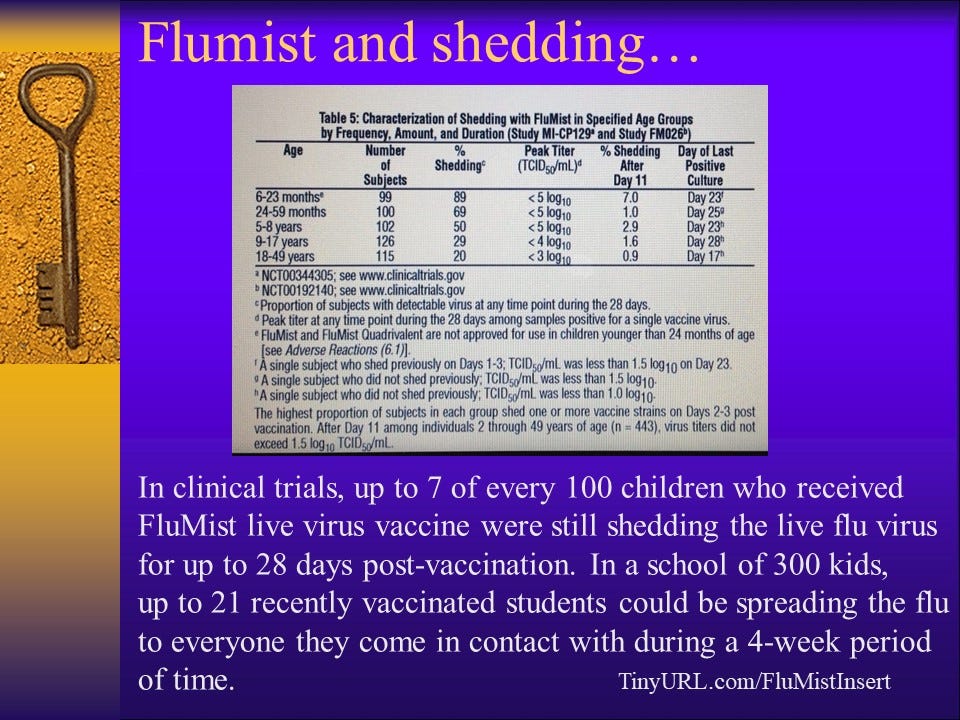
What about the flu shot?
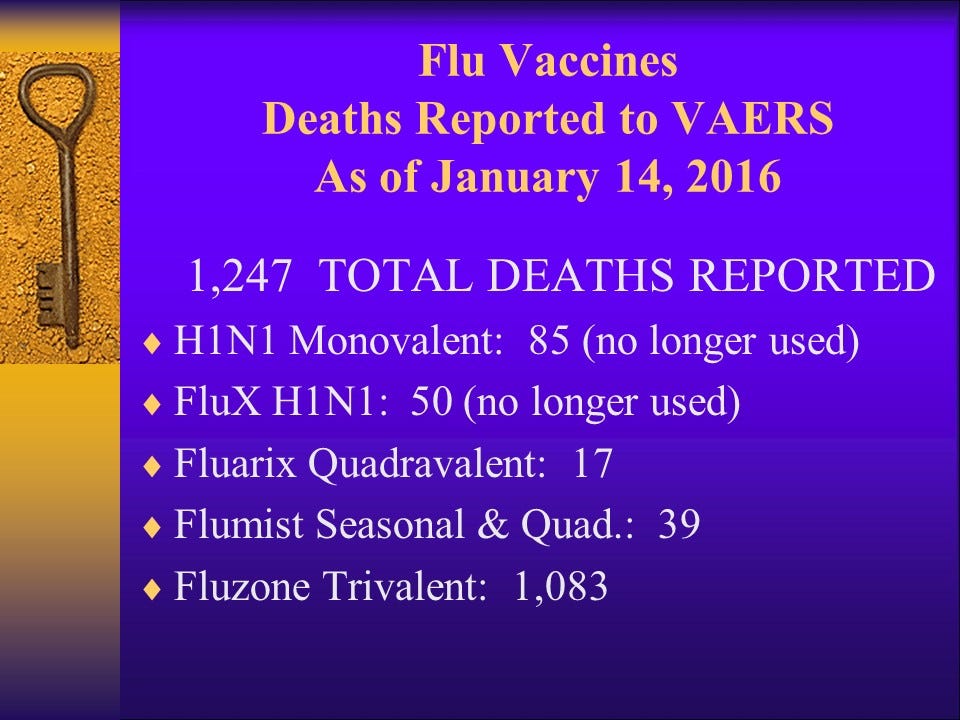
Flu shot deaths from VAERS search, December 11, 2023: Note that the number returned today for Fluzone Trivalent deaths is less than it was when I did this same search in 2016. I don’t know why that would be, but having recently heard rumor that VAERS reports related to COVID-19 vaccines were being deleted from the database, I did a quick search and found this. Is the same thing happening for all vaccine injuries? I don’t know.
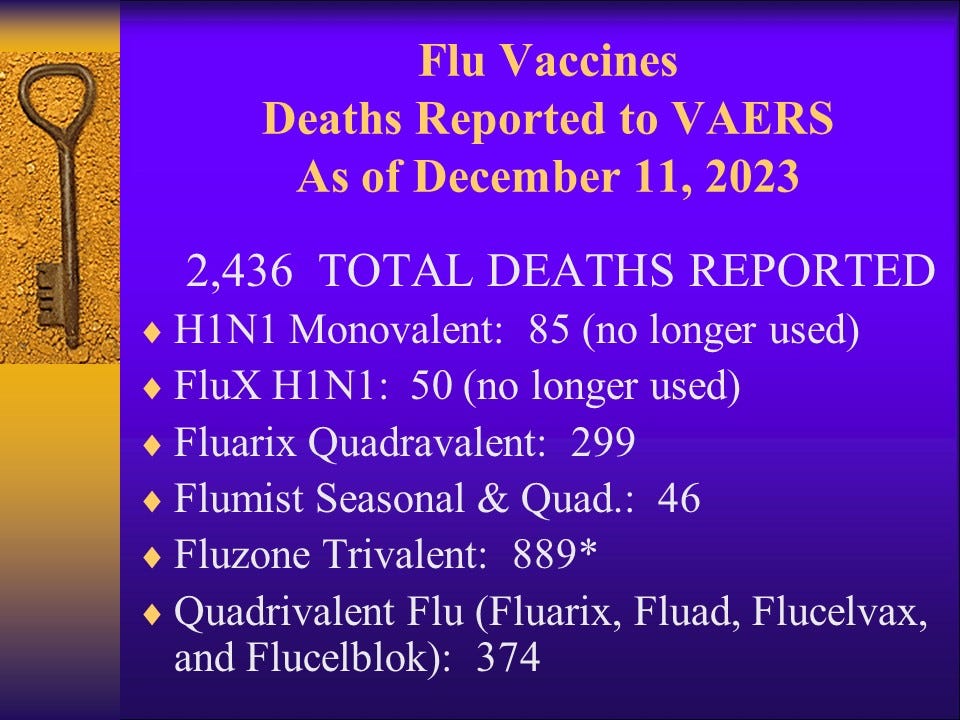
(Source)
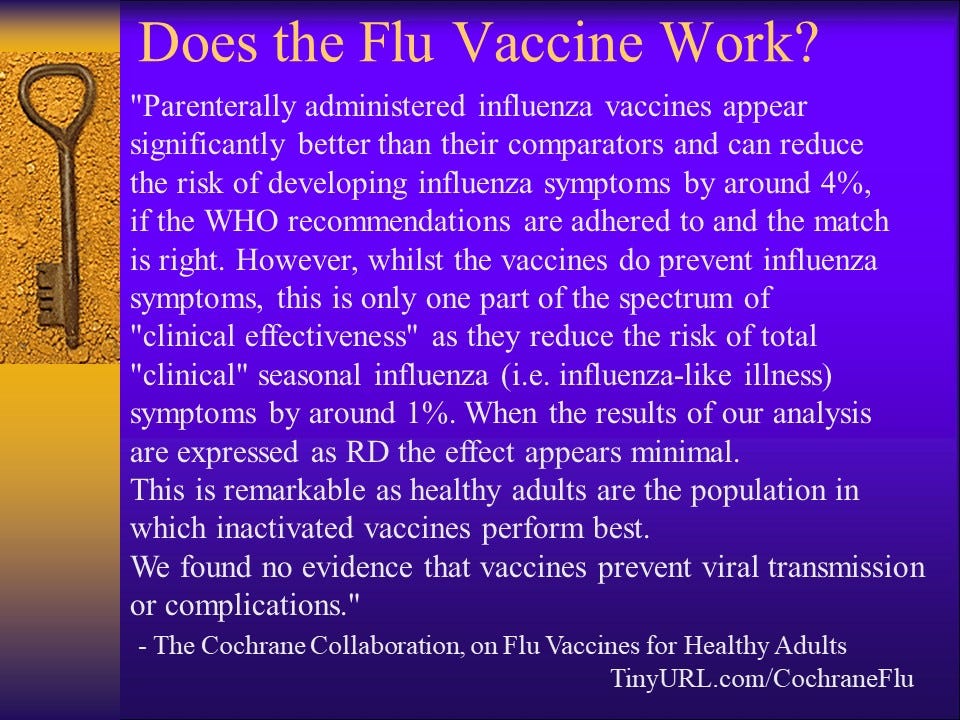
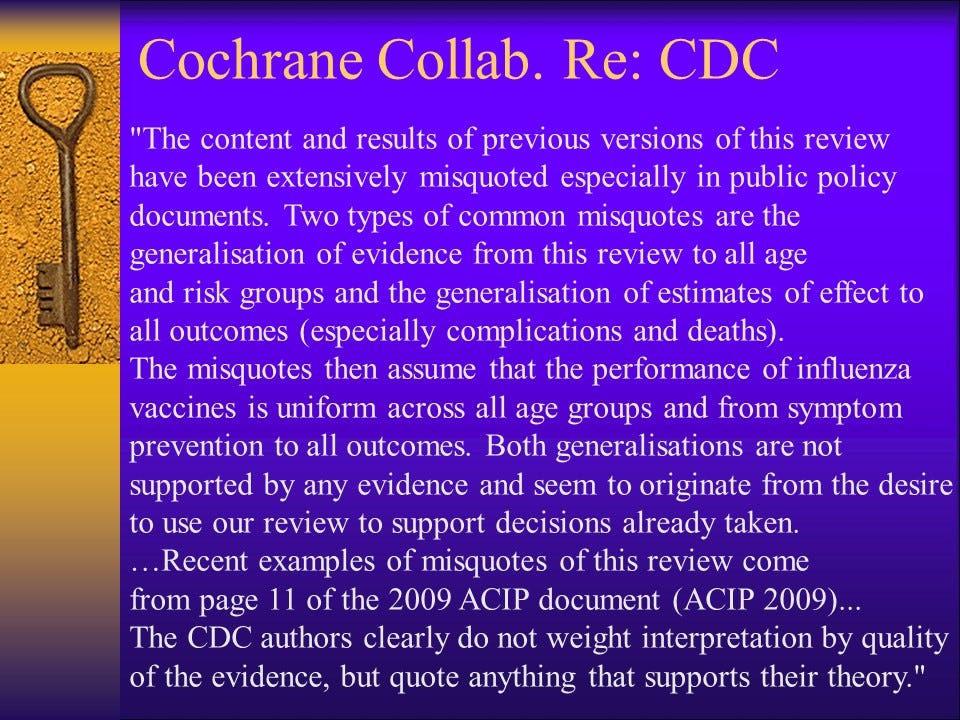
Note: The Cochrane Collaboration’s work on Flu Vaccines for Healthy Adults is an ongoing review. You can read about it here.
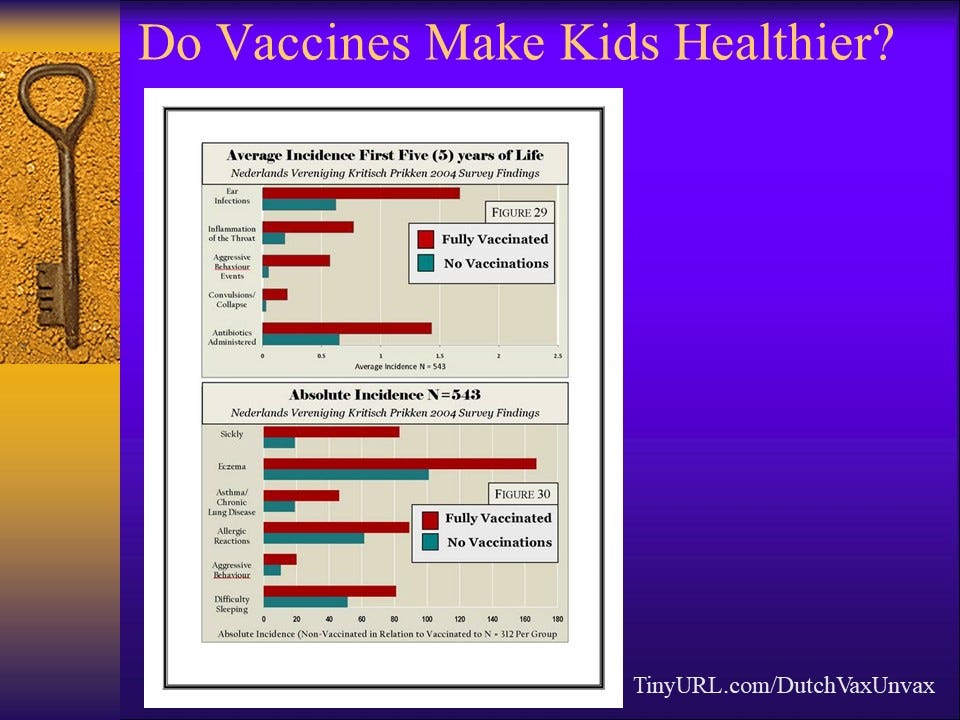
In the above study, conducted in Denmark, children who had received NO vaccinations were compared to Fully Vaccinated children on a number of health outcomes. Without exception, the vaccine-free children were healthier. They had fewer doctors’ visits and hospitalizations. They had fewer episodes of sickness of all kinds and far fewer antibiotics. There was far less eczema, allergies, asthma, ear infections, and throat infections among vaccine-free children. Behaviorally, children who were vaccine free had significantly fewer reports of aggressive behavior. They slept better. They had fewer seizures. They had NO autism.
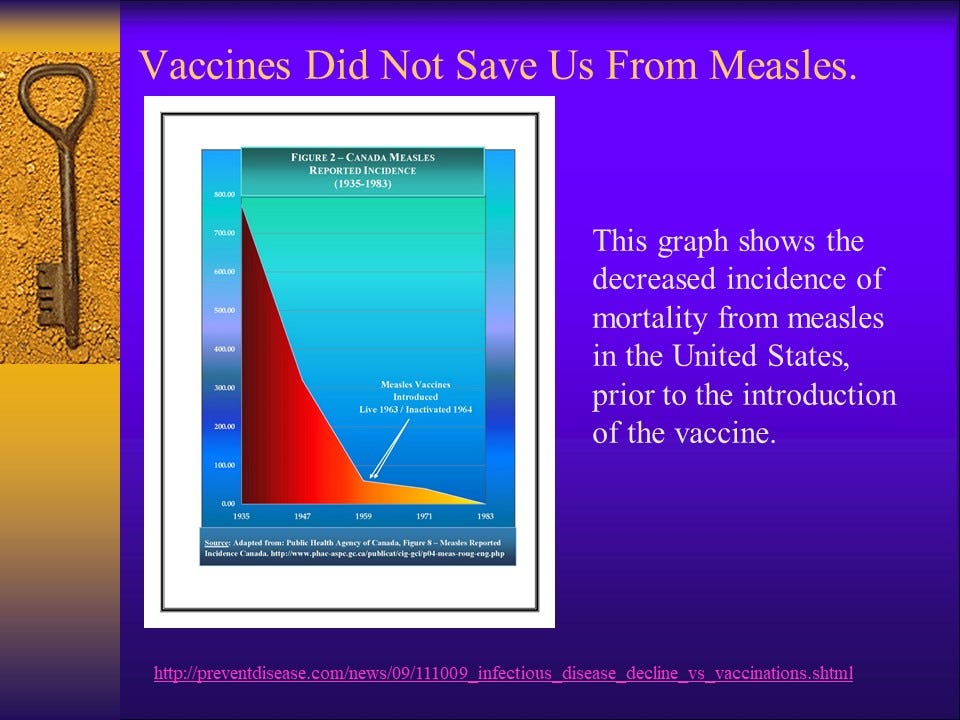
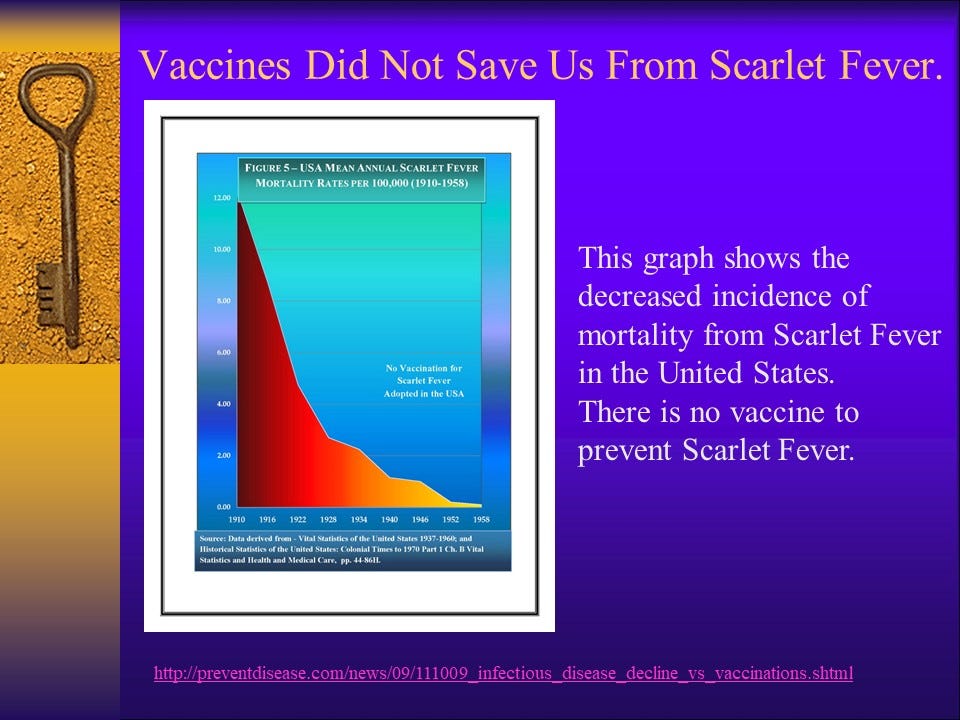
What would it look like if we stopped vaccinating?
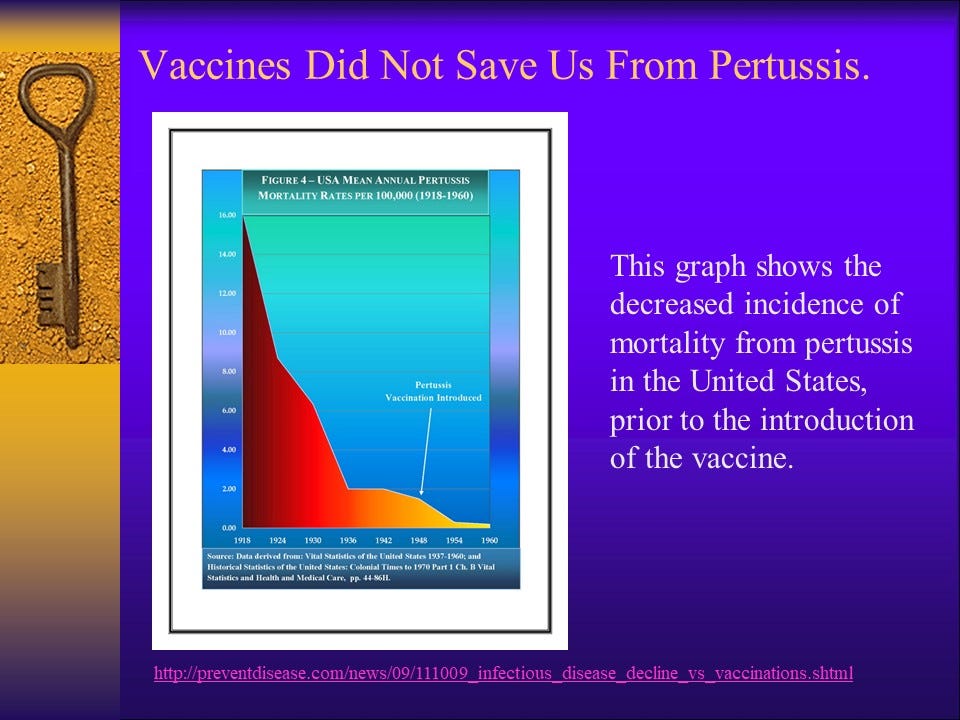
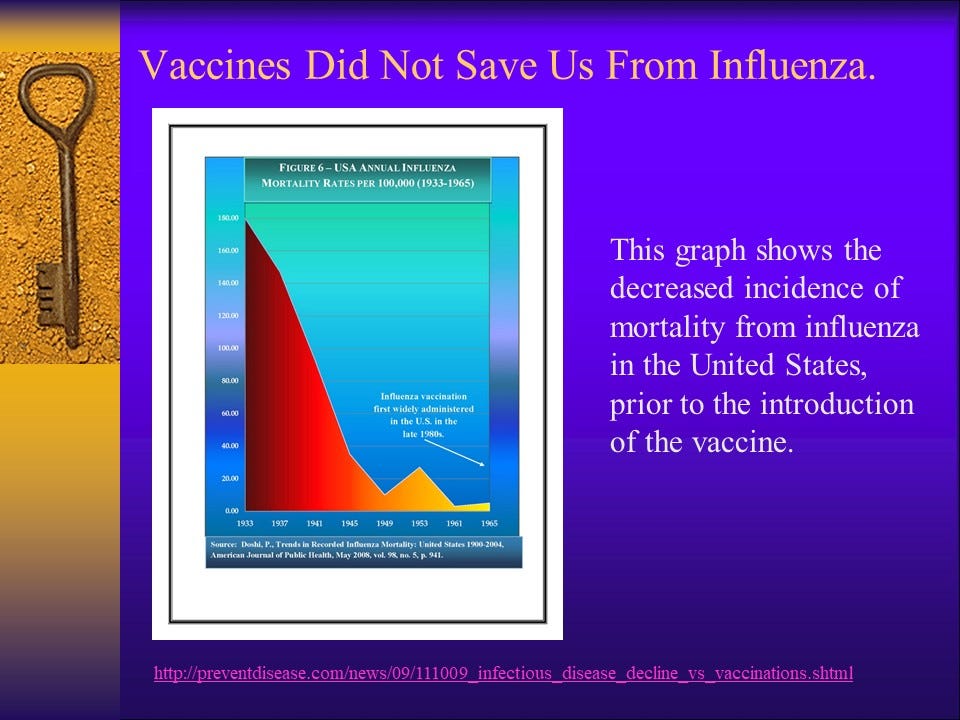
Fear of a world free of vaccines leads people to automatically repeat the mantra that “vaccines have saved us from infectious disease” and “without vaccines we will see a resurgence of deadly childhood infections.”
What does the historical data actually reveal?
For more in-depth analysis of topics covered in this presentation, please check out my other Substack articles: