


Vitamin K Shot and Delayed Cord Clamping
To inject or not? What about oral vitamin K drops?

Many people who are opting out of vaccines also choose to opt out of the vitamin K injection for their newborns. Making informed decisions requires us to become educated about the pros and cons of all medical interventions, especially when it comes to the health and well-being of the most vulnerable among us - our babies. The goal of this article is to help you become more educated about the vitamin K shot, the rationale for its use, the possible reasons you may want to forgo this injection, and some information about alternative methods of supplementing vitamin K in the newborn.
The vitamin K shot is not a vaccine. It is also not “just a vitamin.” Vitamin K injections have been given routinely to basically all hospital-born infants in the United States since the 1970s. Vitamin K shots are given to help prevent something called Vitamin K Deficiency Bleeding (VKDB), which is a rare, but serious medical emergency that can lead to disability or death.
The problem of bleeding into the brain occurs mainly from 3 to 7 weeks after birth in just over 5 out of 100,000 births (without vitamin K injections); 90% of those cases are breastfed infants (3) because formulas are supplemented with unnaturally high levels of vitamin K. Forty percent of these infants suffer permanent brain damage or death.
The cause of this bleeding trauma is generally liver disease that has not been detected until the bleeding occurs. Several liver problems can reduce the liver's ability to make blood-clotting factors out of vitamin K; therefore extra K helps this situation. Infants exposed to drugs or alcohol through any means are especially at risk, and those from mothers on anti-epileptic medications are at very high risk and need special attention. (source)
Is there a high amount of aluminum in the vitamin K shot?
Aluminum in vaccines has become a big topic among my circle of friends, and understandably so. If you have read my previous post about the 800 pound aluminum gorilla, you will understand why so many people are concerned about aluminum, especially at the levels being injected into tiny babies. I believe it is in part due to this concern that many people also believe there is a high level of aluminum in the vitamin K shot. This is not the case. While it is true there is SOME aluminum in the vitamin K shot, aluminum is not the only, or even the biggest issue we need to worry about.
For those who have been convinced there is 100 mcg. of aluminum in the vitamin K injection, I hope you will continue reading. There are other, very important concerns regarding the vitamin K injection, and we need to be sure we are sharing accurate information. When you incorrectly tell a pregnant woman, "Vitamin K shot has 100 mcg. of aluminum," her doctor will quickly be able to dispel that myth. That may lead to the mother allowing administration of Vitamin K, because she doesn't understand the REAL dangers involved. It may also cause her to doubt everything else you tell her about vaccines.
Preservative Free does not mean there are no issues.
When a doctor tells you, "We have a preservative free version," of the vitamin K injection he/she is referring to Amphastar. Please do not assume that because it is "preservative free" it is "safe." In this instance, being “preservative free” means that Amphastar contains no benzyl alcohol, unlike Hospira, which has 9 mg. of benzyl alcohol.
The benzyl alcohol in Hospira has been associated with toxicity in newborns, known as “gasping syndrome.” Gasping syndrome is characterized by metabolic acidosis, encephalopathy, intracranial hemorrhage, and respiratory depression with gasping. Alcohol is a central nervous system depressant and gasping syndrome is a result that has been most often associated with pre-term infants. Because all infants are treated exactly the same when it comes to vitamin K injections and vaccines, the effect of 9 mg. of benzyl alcohol in a preterm, low-birthweight infant would be expected to cause more issues than it would for a full-term, robust baby. However, it should be noted that these severe, adverse reactions have also occurred in full-term infants of normal birth weight and without any known risk factors beforehand. Because of the issues with benzyl alcohol in Hospira, the preferred option in recent years has been Amphastar.
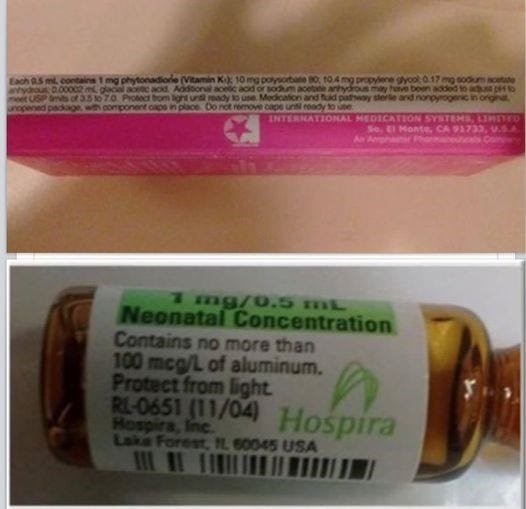
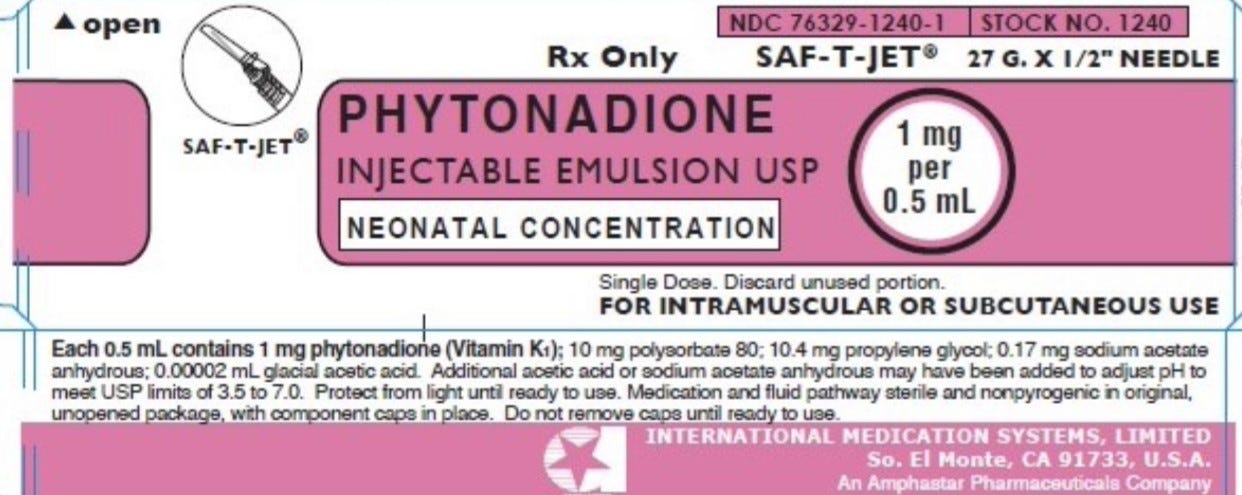
The photo above shows Amphastar and Hospira. These are two different Vitamin K Injections, given to newborns.
What I want to point out is that Amphastar's formulation contains Polysorbate 80. It’s the second ingredient listed, with 10 mg. per dose.
Concern: polysorbate 80 and Premature Ovarian Failure
In January 2016, The American College of Pediatricians issued a statement indicating their concern about the amount of Polysorbate 80 in the HPV vaccine and the increased risk of infertility from premature ovarian failure (POF). Each dose of Gardasil contains 50 mcg. of Polysorbate 80. Amphastar Vitamin K injection contains 200 TIMES the amount of Polysorbate 80, when compared to Gardasil. What do you suppose that is doing to the future fertility of our children?
Concern: polysorbate 80 and Blood Brain Barrier permeability
Polysorbate 80 is also used in research to increase the permeability of the Blood Brain Barrier (BBB) - not a good thing when you are talking about babies whose BBB is already not completely impermeable. It’s especially concerning when you realize that the vitamin K shot is given within minutes of birth and is most often followed very closely by the hepatitis B vaccine, which contains 250 mcg. of aluminum. Opening the blood brain barrier and allowing aluminum to enter is not a good thing and anyone who tells you it is, definitely does not have your baby’s best interest as a top priority.
Hospira LOOKS like it contains 100 mcg of aluminum. It does not. The label reads "no more than 100 mcg of aluminum per LITER." Each dose is .5mL (1/2 milliliter). There are 1,000 mL in 1 Liter. At 100 mcg/L, you would have to inject TWO AND A HALF LITERS of the Hospira Vitamin K to reach the same level of aluminum (250 mcg.) that IS injected on the first day of life when an infant receives the Hepatitis B vaccine.
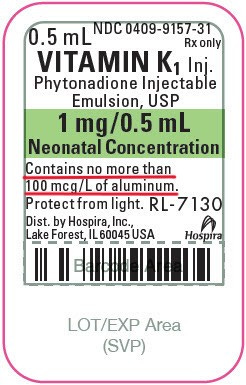
ALUMINUM is NOT the main problem. The problem with Hospira is that it contains 9 mg. benzyl alcohol, which can tax the liver and may contribute to the high frequency of infants who develop jaundice within two days of birth, in addition to previously mentioned concerns about gasping syndrome in preemies.
What IS VERY interesting about this is that the Hospira vial contains the information about aluminum at all. That's because aluminum is limited in injectables to 5mcg/kg of body weight administered over a 24-hour period, because at higher doses it causes kidney failure and brain damage. The information on the Vitamin K Injection is there because it is NOT a vaccine. Vaccines are exempt from the rule about aluminum in other injectables. That’s because vaccines, even though they are given to individual babies, are not considered a prescription medication; they are considered a public health measure, so they are exempt from the rules governing other medications your babies and children may receive. With vaccines, it’s all about “the greater good,” which means if anyone is going to look out for the individual health and well-being of YOUR child, it has to be YOU.
The Hospira Package Insert does not list Aluminum among the ingredients; however, there is a warning on page 3 of the insert about the fact that it does contain aluminum. This is because it is given to very low birth weight babies with poor kidney function, and ALL sources of aluminum are supposed to be carefully tracked. (They just exempt the vaccines from the total calculated.)
When you look at the insert, you will notice it has a Black Box Warning.
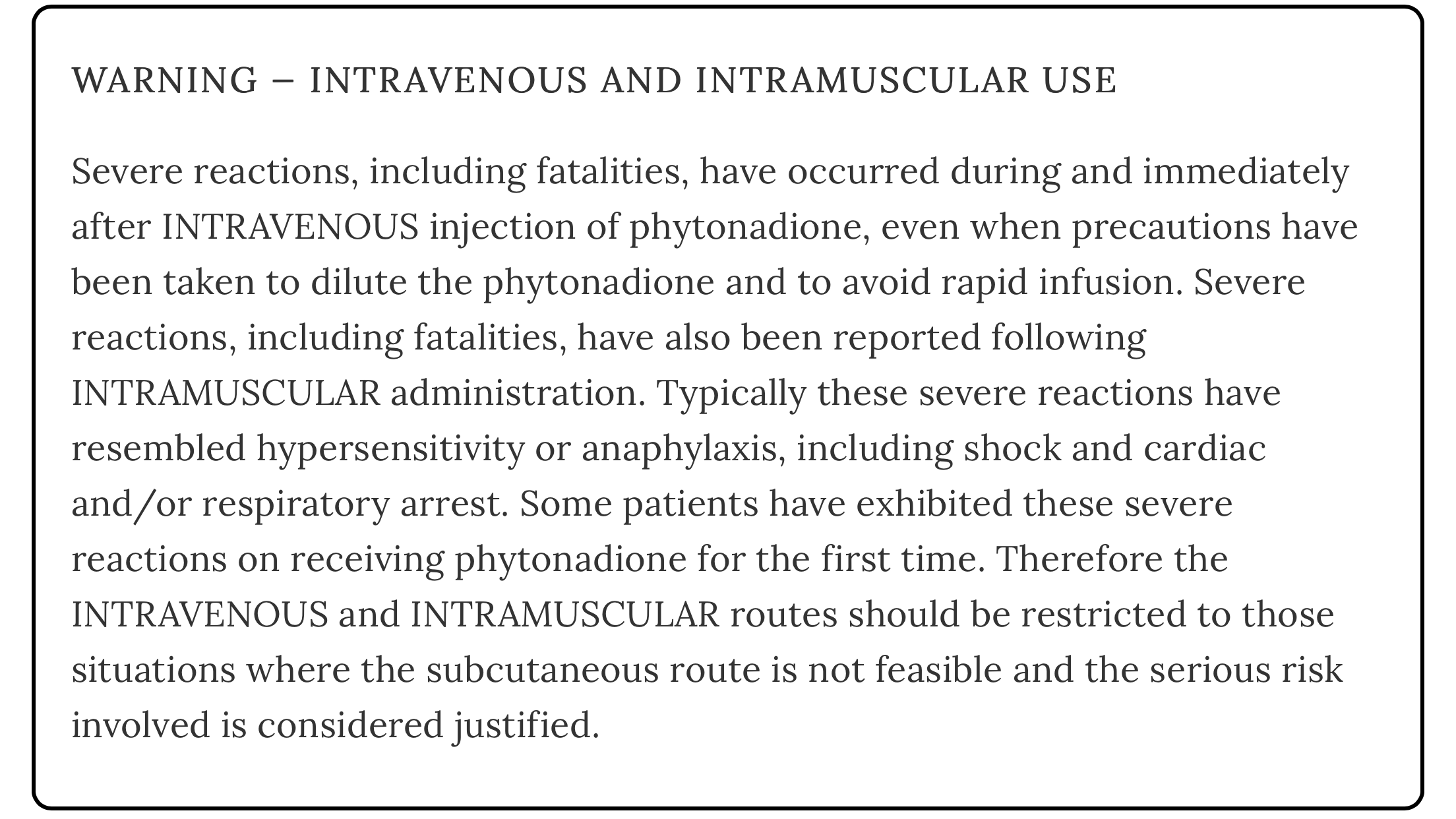
Boxed warnings (also known as black box warnings) are the strictest warning that can be issued for a drug by the Food and Drug Administration (FDA). First implemented in 1979, they are there to alert doctors to a potentially serious side effect of a medicine or to restrictions on the use of a medicine.
From the review Characterizing the Severe Reactions of Parenteral Vitamin K1:
The prescribing information for vitamin K1 emulsion notes that injection site pain, transient flushing, taste disturbance, and cutaneous reactions have been reported. Rare instances of dizziness, rapid and weak pulse, sweating, hypotension, dyspnea, and cyanosis are also addressed. Benzyl alcohol has been associated with toxicity in newborns, termed ‘‘gasping syndrome,’’ characterized by metabolic acidosis, encephalopathy, intracranial hemorrhage, and respiratory depression with gasping. Vitamin K1 has a boxed warning about the possibility of severe reactions, including fatalities, with IV and IM administration. These reactions resemble hypersensitivity or anaphylaxis, including anaphylactoid reaction, and have led to shock and cardiac and/or respiratory arrest. Unfortunately, they are not well understood or characterized. It has been suggested that the reaction occurs as a result of vitamin K1 itself and/or as a result of the polyoxyethylated fatty acid vehicle. Although adequate dilution, appropriate dosing, and slow administration have been thought to minimize these reactions, reactions have still been reported despite those precautions.
Does the vitamin K shot increase the risk of childhood leukemia?
The answer to that question is, possibly. In the 1990s, there were some journal articles published linking vitamin K injection at birth to increased risk of childhood leukemia. Most mainstream sources now discredit those papers, noting that there have been multiple other studies which found no connection. The issue has to do with the very tight control of vitamin K production, which naturally occurs at a slow rate following birth. Research has indicated that this tightly controlled level of vitamin K is very likely not a mistake in the design of little humans. The amount of vitamin K in infants helps to regulate the rate of cellular division, and the research supporting a link between vitamin K injection and leukemia found that the very large dose of vitamin K given through injection at birth dysregulated that process, and that was what led to the increase in leukemia. This is a good article where you can read more about that and access the study citations.
Given that the vast majority of mainstream doctors and even midwives recommend the vitamin K shot, and some places even require it for all hospital births, those parents who want to make the best decisions for their children NEED to research this issue from all points of view in order to make informed choices and birth plans.
It’s important to note that not all doctors agree with the mainstream. Here is a really good article from Dr. Ben Kim, in which Dr. Kim discusses the process he and his wife went through in deciding to forego the injection for their second child. Dr. Kim provides the text of a great article from Dr. Linda Palmer. I am providing the link to Dr. Palmer’s article on her website, which has a lot of other great information you might want to check out.
What about oral vitamin K?
The history of vitamin K administration in the United States is discussed in an article from holistic midwife, Jan Wolfenberg. Her write-up on vitamin K is definitely worth reading, saving, and printing. Ms. Wolfenberg writes:
The fact that babies are born low in vitamin K was discovered in the early-mid 1900’s. There were a couple of U.S. childbirth practices happening at the time that caused undue stress on babies. One was the fact that most women were being completely knocked out for delivery, and since they couldn’t push, the babies were being pulled out by forceps – like metal salad tongs applied to the sides of baby’s head and then traction placed to literally PULL the baby out. This obviously resulted in lots of trauma to those babies’ heads, both inside and outside the skull. At the same time, it was the height of infant circumcision. Virtually all baby boys were being circumcised within hours of birth, which was surely another big trauma. And what they observed was increased bleeding, difficulty getting bleeding to stop, in babies with these traumas. Blood tests revealed the new information that babies were born with 20-50% of the blood-clotting activity of adults, including the vitamin-K-dependent factors. Viewing this as a design flaw (during the era when it was deeply believed that Nature was faulty and needed to be improved upon), modern medicine quickly came up with a solution – give all babies a dose of vitamin K at birth.
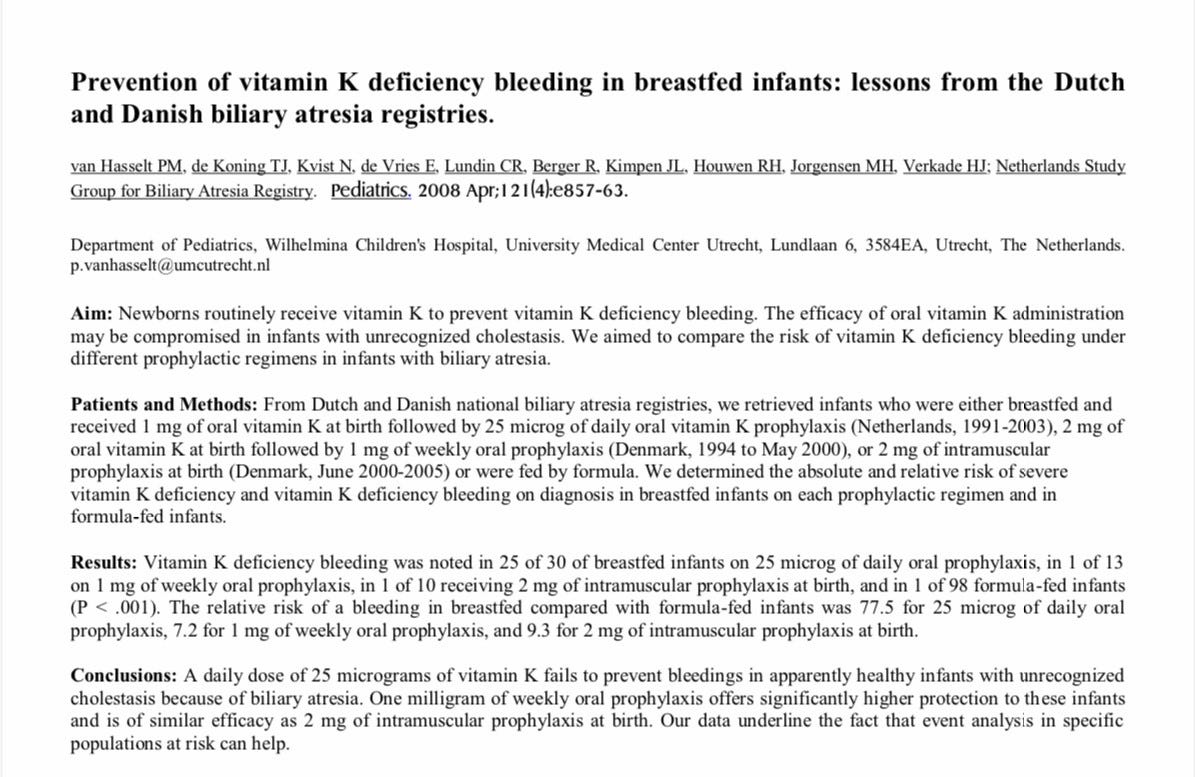
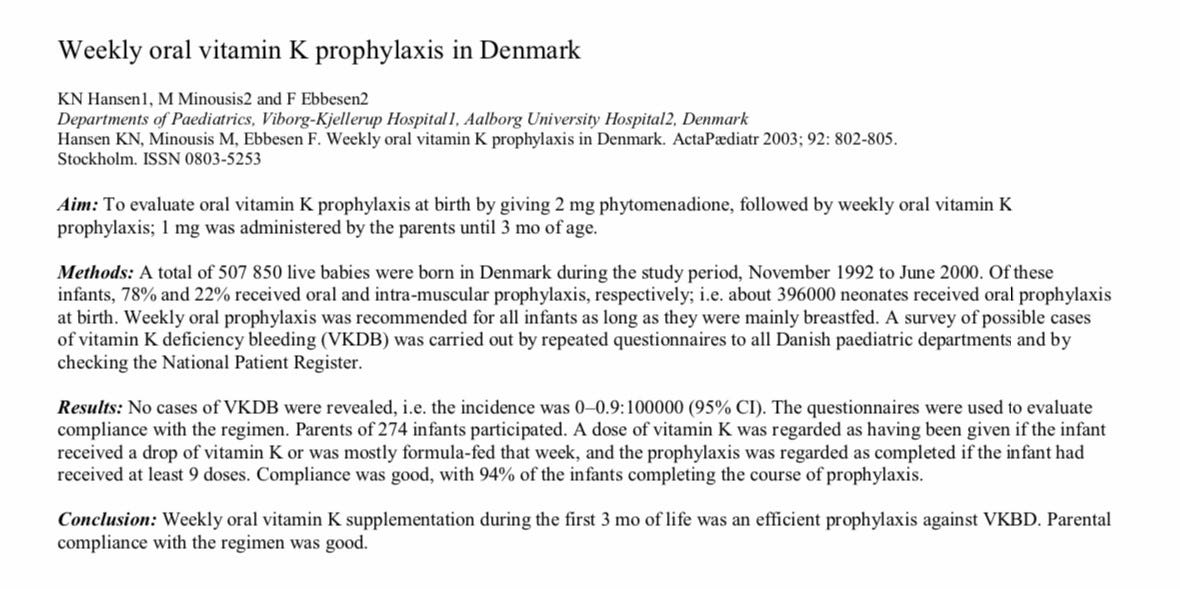
Initially, in the 1940s vitamin K supplementation in the United States was accomplished via oral vitamin K drops. However, there were problems with hemolytic anemia and jaundice because the doses being used were too high. The injectable form of vitamin K was licensed in 1961 and its use was nearly universal by the 1970s. Because of the previously mentioned concerns about increased risk of leukemia from the injection, many countries stopped using it in the 1990s and went back to using oral supplementation. (The United States continued to advocate for vitamin K injection as the sole option.) There have been several protocols developed in different countries, with the most effective according to research being the Dutch and Danish protocols, which provide protection against Vitamin K Deficiency Bleeding (VKDB) that is comparable to what is conferred via injection.
If you are looking for specific recommendations for oral vitamin K products and dosing, please see page 5 of this document. And please read ALL of the information, which includes excellent data on the three types of Vitamin K Deficiency Bleeding (VKDB). There are some situations in which the risk of intercranial bleeding is elevated, including if the mother is taking anti-seizure medications, and in the case of drug/alcohol exposure to the infant in utero. Having all of the available information is important when making informed decisions.
Here is some information on vitamin k, from Stanford Medical School, just so you have more than one source to consider.
Delayed cord clamping and stem cells…
As I have hinted in the title of this Substack post, there is an association between the vitamin K injection and the practice of clamping the umbilical cord after birth, and that association has to do with the baby’s stem cells.
The following video from Dr. Suzanne Humphries is a good place to start for gaining understanding of how these issues are related:
As Dr. Humphries tells us, the process of being born is one in which the baby, and particularly the baby’s head, is squished (to use a technical term) while descending through the birth canal. When the baby is born, modern hospital practice is to cut the umbilical cord immediately, which robs the baby of 40% of his or her own blood, and also robs the baby of the stem cells that are provided naturally, and which help to heal any damage that occurs during the birth. Additionally, because the very high level of vitamin K injected (many times higher than what would be available naturally) thickens the blood, it makes it difficult for those stem cells that are left to get where they need to be.
One thing I find interesting is that more people, and specifically, more doctors, are not talking about the benefits of delayed cord clamping.
Currently, most hospitals in the United States practice early (immediate) cord clamping. This means cutting the umbilical cord 10 to 15 seconds after birth or sooner.
Before the mid-1950s, it was standard practice to wait one to five minutes before cutting the cord. Around this time, the number of births in hospitals began to rise.
Research didn’t link specific benefits to a delay in clamping. It was believed early clamping could keep mothers from losing too much blood. So, healthcare providers began clamping sooner after birth.
In recent years, more research has called attention to how waiting to clamp the cord may benefit babies more. (source)
This article gives a good overview of the benefits of delayed cord clamping, and under what circumstances it might not be possible (such as in the case of maternal hemorrhage).
The benefits of delayed cord clamping have been known for centuries.
In the early 19th century, the English physician, Erasmus Darwin mentioned “another thing very injurious to the child is the tying and cutting of the navel string too soon, which should always be left till the child has not only repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much weaker.”
Obviously, it makes sense that waiting until the umbilical cord stops pulsating and turns white is beneficial to the baby. The research indicates it not only helps heal any birth trauma by making sure the baby actually gets his or her own stem cells, but there is also strong evidence that delayed cord clamping protects the baby against iron deficiency anemia during the first six months of life. This is not a small thing, as iron-deficiency anemia is a big problem contributing to the epidemic of learning disabilities and neurodevelopmental delays in children. A 2015 study found:
Delayed CC compared with early CC improved scores in the fine-motor and social domains at 4 years of age, especially in boys, indicating that optimizing the time to CC may affect neurodevelopment in a low-risk population of children born in a high-income country.
Given the benefits of delayed cord clamping, one is left wondering why the practice is not widely promoted in the hospital setting. One reason is money. Stem cells are “the future of medical research.” And since laws protecting the fetus make it difficult for medical researchers to obtain fetal stem cells, those researchers are practically salivating to get their hands on umbilical cord stem cells (and everything else they might possibly be able to take).
Stem cells are the next frontier in medicine. Stem cells are thought to have great therapeutic and biotechnological potential. This will not only help to replace damaged or dysfunctional cells, but also rescue them and/or deliver therapeutic proteins after they have been engineered to do so. Currently, ethical and scientific issues surround both embryonic and fetal stem cells and hinder their widespread implementation. In contrast, stem cells recovered postnatally from the umbilical cord, including the umbilical cord blood cells, amnion/placenta, umbilical cord vein, or umbilical cord matrix cells, are a readily available and inexpensive source of cells that are capable of forming many different cell types (i.e., they are “multipotent”). (source)
If parents choose to support medical research by allowing immediate cord clamping and if they are making an informed choice to donate their infant’s blood and stem cells, that’s one thing. It’s another thing for hospitals to engage in theft of babies’ stem cells and blood in order to sell the remains to the highest bidder for research purposes without the parents’ knowledge or consent. I was not able to find evidence about hospitals selling (vs. “donating”) umbilical cord blood. Honestly, I didn’t take the time to research that aspect. What I did find is that the Federal Government has invested heavily in non-embryonic stem cell research, to the tune of several billion dollars (source).
And I found this:
Researchers can go to this website and order human cord blood for anywhere from $910.00 to $2,577.00 (U.S) per vial. Someone is obviously making lots of money from stem cells and cord blood that rightfully belongs to the babies from which they were stolen. Because parents didn’t know better. It is my hope that after reading this article, you now know better. Because when we know better, we do better, and when it comes to the health of our precious babies, nothing is more important than making truly informed choices.
The way things are going I am of the opinion that it is safest to avoid all health professionals and have your baby in private at home without interference.
Wow thank you
I feel we should always get all our products information before deciding wether to use it
Seems common sense