

Meningococcal Infection CAUSED by Meningococcal Vaccination - what the VAERS data tells us.
Meningococcal Infection CAUSED by Meningococcal Vaccination - what the VAERS data tells us.
Should your teenager get this shot for college? Read this first!

I have written about Meningococcal infection and vaccination a few times in the past. The first time I wrote about it was in 2011. I updated and expanded on that post (from VaxTruth) and added it to my Substack last year. With the added interest at this moment, resulting from the attention being given to the case of Alexis Lorenze, I wanted to republish the information and expand on it, yet again.
Meningitis, or meningococcal infection is something that terrifies parents probably more than just about any other illness, except possibly, cancer. Even among my friends who are adamantly opposed to vaccinating for things like polio, measles, flu, pneumonia, and chickenpox, the fear of meningitis can cause them to waffle in their commitment to keeping their children vaccine-free. And it’s no wonder when we see campaigns like this one.

The stories in the Voices of Meningitis video are heart-breaking. One question I have about these cases is if those whose stories are told were fully vaccinated? I wonder how many of those cases occurred in children AS A RESULT of being vaccinated with the Meningococcal vaccine. When I visited the Vaccine Adverse Events Reporting System (VAERS) today, what I wanted to know was, among the fewer than 1% of vaccine reactions that are reported to VAERS, how many of the reactions for the meningococcal vaccines listed meningitis as an adverse reaction.
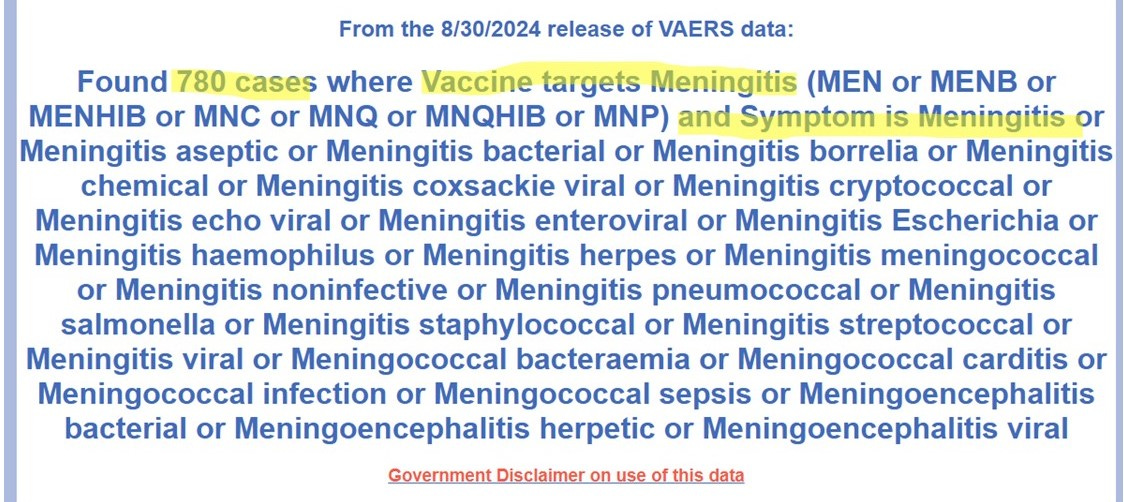
My query, which was restricted to meningitis as a symptom, returned 780 cases. (Note: When I first wrote this article in 2011, there were 103 cases.)
Here are a few of the details:
VAERS ID 160698: An 18-year-old female received the meningococcal vaccine.
Write-up: On 8/1/00 approximately 2 weeks post vax, the pt developed a fever, myalgia, stiff neck and arthralgias. After approximately 24 hours of developing the above symptoms, the pt developed a diffuse non-pruritic macular rash on her lower legs, which spread to her abdomen and upper extremities. The pt was seen initially in the clinic and thought to have a viral infection and symptomatic care was advised at that time. Over the next 48 hours the pt symptoms increased in severity and the pt experienced a syncopal episode. She was then seen in the ER and that time transferred to the hospital where she underwent a lumbar puncture. The pt was diagnosed with bacterial meningitis and treated accordingly.
Died? No.
VAERS Case 170356: 53-year-old male, vaccinated against meningococcal disease:
Write-up: It was reported that an adult male pt received a Menomune A/C/Y/W-135 vaccination on 3/6/00. Reportedly, the pt died on 4/14/00. dx’d with purulent meningitis. Autopsy done at medical examiner’s office. Further medical follow-up is requested and ongoing. On 05/22/2001, the autopsy and medical examiners reports were received. Autopsy report revealed the following findings from the head and central nervous system. “The leptomeninges overlying the frontal lobes have yellow-green opacified material present, consistent with purulent meningitis process.” From the correspondence received from a physician it was stated “This case was associated with large numbers of gram-positive diplococci having the morphology consistent with S. pneumonia. A silver stain and a PAS did not support the presence of any other organism.”
Died? Yes.
VAERS Case 200387: 19-year-old female vaccinated against meningococcal disease:
Write-up: From initial information at manufacturer, it was reported that a 19-year-old female patient received Menomune A/C/Y/W 135, UB034AA, on 7/2/01. Route/site were not reported. Patient had cultures sero group C. On 2/15/03, patient had blood cultures and was positive for ? of meningitis group C. Patient was hospitalized for 4 days, then died on 2/18/03.
Died? Yes.
Given the large amount of interest in the case of Alexis Lorenze, I am receiving even more messages than usual from parents who are concerned that their children are being “required” or “mandated” to receive the meningococcal vaccine in order to attend college and/or to live in the dorms. I got one of those messages this morning. It was the first thing I saw when I opened up my laptop.
Hi Marcella. I hate to ask you this, but my oldest is off to college next year and she wants to go to the University of Kentucky, and they require the meningitis vaccine. Michigan allows exemptions. I don't know if Kentucky does. What should I do if I am forced to give her the shot??? …meningitis quadrivalent ACWY vaccine…This is the one they require. Should she have this one? What are your thoughts?
My thoughts:
1. Kentucky does have religious exemptions, just like Michigan does, and those religious exemptions apply for college. Here is where you can find out more about the laws in your state. I advised this mom to sign up at the NVIC Advocacy Portal and join the Kentucky state team. Because vaccine exemption laws differ by state, and because the laws are changing rapidly, it is important to be sure you get the most accurate information. The state teams will know best what’s going on in each state. Here is where you can find and join the team for your state.
2. In response to the question, “What should I do if I am forced to give her the shot???” This may sound brutal to some. That is intended. If my adolescent or young adult child wanted to attend a college that did not allow her the legal right to religious exemption from vaccination, I would not pay for her to attend that school. Period. I would not co-sign for student loans, and I would not help her with the financial aid application. If she insisted on attending that particular school, and if she insisted on going forward with vaccination, I would not help her in any way to accomplish those goals. Knowing what I know about vaccination at this point, I would do everything possible to educate my child about the danger to her life if she chose to pursue that path. Just as I would if my child were experimenting with illegal drugs or engaging promiscuous sex. It is my job as a parent to educate and empower her to make informed decisions about health behaviors. Vaccination is no different. If my child decided to use heroin or fentanyl, I would not drive her to the parts of town where she could score her fix, and I would not pay for an Uber so she could do it on her own. I would not pay for a hotel room so she could have sex indiscriminately. And I would not invest tens of thousands of dollars in an institution that will strong-arm her into injecting vaccines that may kill her, and which may end up giving her the same strains of meningitis the vaccines are advertised to prevent.
Currently, there are five states that do not allow for religious exemptions from vaccination. They are: California, Connecticut, Maine, New York, and West Virginia. In an interesting turn of events, the University of California system just last week has reversed their policy on vaccination exemptions after two successful lawsuits filed by ICAN and attorney Aaron Siri. Here is where you can learn more about that. As for the other states, I strongly suggest boycotting. There are plenty of other places to send your children and your money.
Because of the increased interest in this topic, and especially as regards the meningococcal vaccine, I spent some time this morning looking at the data in the Vaccine Adverse Events Reporting System (VAERS). The last section of this article will present my findings from that effort. The next section will give you some information that you need to help you understand just why meningitis happens more often in certain age groups, and what you can do to reduce the chances of it happening to your child.
As noted previously, the results of my initial query revealed there have been 780 cases of vaccine-induced meningitis/meningococcal infection after meningococcal vaccination reported to VAERS. A 2011 study commissioned by the United States Department of Health and Human Services to investigate the accuracy of reporting to VAERS found that less than 1% of even the most serious vaccine adverse events - including deaths - are reported. So, the actual number of serious adverse events that included “meningitis” from the meningococcal vaccination is more likely to be in the range of about 78,000. That’s a pretty big number. What you need to know, in order to make an informed decision, is just how likely it is that your child will contract meningitis if he or she is not vaccinated.
I printed out the CDC’s report - Prevention and Control of Meningococcal Disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP). The report is long, and full of lots of scary statistics. It is clearly designed to give the impression that meningococcal infection is monstrous and you, as a parent, MUST vaccinate your children in order to protect them from the horrors of this very preventable illness. I say “preventable” because meningococcal infection IS preventable, and it appears that the BEST prevention is to REFUSE vaccination!
Here is what I have learned:
According to the CDC Report, there was a yearly average of 360 cases of meningococcal disease in the United States between 2015 and 2018. 2020 Census data indicates the U.S. population is 331,449,281. This means meningococcal infection occurs in 1 person out of every 920,692 people, or 0.0001086139%% of the population.
According to the CDC, the case-fatality ratio for meningococcal disease is between 10-15%. This means that each year in the U.S. it is estimated that between 36-54 people die from meningococcal infection. This translates to an annual death rate in the U.S. of approximately 0.00000015; or about 1.5 deaths per 10 million people. Way less than “one in a million.”
“During 1991-2002, the highest rate of meningococcal disease (9.2/100,000) occurred among infants; the rate for persons aged 11-19 years (1.2/100,000) also was higher than that for the general population.” (CDC, MMWR, vol. 54, No. RR-7, p. 2)
“U.S. surveillance data from 1998-99 school year indicated that the overall rate of meningococcal disease among undergraduate college students was lower than the rate among persons aged 18-23 who were not enrolled in college.” Rates were higher among freshmen, and highest among freshmen living in dormitories. (CDC, MMWR, vol. 54, No. RR-7, p. 3)
“Persons who have deficiencies in the terminal common complement pathway (C3, C5-9) and those with anatomic or functional asplenia are at increased risk for acquiring meningococcal disease. Antecedent viral infection, household crowding, chronic underlying illness, and both active and passive smoking also are associated with increased risk for meningococcal disease.” (CDC, MMWR, vol. 54, No. RR-7, p. 2).
We need some definitions and understanding of what causes increased risk for infection from meningococcal infection in order to understand WHY infants and children are more vulnerable than the general population.
Definitions from the Medical Dictionary:
(Caution: If technical information makes your eyes glaze over, you may want to either skim or skip the definitions. The translation of the definitions is basically that the immune system works together and if you upset one part of it there is a domino-effect, resulting in increased vulnerability to illness from a variety of sources.)
Complement: Immunology adjective Pertaining to the complement system noun
1. Any protein of the complement system
2. Complement system
The term was first used for a heat labile factor in serum that caused immune cytolysis of antibody coated cells; it now refers to the entire functionally related system comprising ± 25 distinct serum proteins, which mediate the nonspecific inflammatory response to various antigens through a complex sequence of enzymatic cleavages; complement is thus the effector not only of immune cytolysis but also of other biologic functions; it is activated by 2 routes, the classic and alternative pathways.
Complement: a complex series of enzymatic proteins occurring in normal serum that are triggered in a cascade manner by, and combine with, the antibody-antigen complexes, producing lysis when the antigen is an intact cell. Complement comprises 25 to 30 discrete proteins, labeled numerically as C1 to C9, and by letters, i.e. B, D, P, etc., and with C1 being divided into subcomponents C1q, C1r and C1s. Components C3 and C5 are involved in the generation of anaphylatoxin and in the promotion of leukocyte chemotaxis, the result of these two activities being the inflammatory response. C1 and C4 are involved in the neutralization of viruses. The components also combine in various sequences to participate in other biological activities, including antibody-mediated immune lysis, phagocytosis, opsonization and anaphylaxis. The complement system is known to be activated by the immunoglobulins IgM and IgG.
alternate complement pathway, alternative complement pathway: the sequence in which complement components C3 and C5 to C9 are activated without participation by C1, C2 and C4 or the presence of an antibody-antigen complex.
complement cascade: the sequence of reactions, each being the catalyst for the next, that leads to the terminal complement pathway and cell lysis. There are two pathways for activation of C3, the ‘classical’ (below) and the ‘alternate’ (above).
classical complement pathway: the one in which all of the complement components C1 to C9 participate and is triggered by antibody-antigen complexes.
complement deficiency: various complement components may be deficient without serious effects on the host. C3 deficiency is most severe and occurs in humans, Brittany spaniels and Finnish-Landrace lambs. Increased susceptibility to infections results.
Terminal Complement Pathway: the final stages of complement activation in which C5, C6, C7, C8 and C9 are activated; common to both the alternate and classical pathways.
End of definitions… back to the discussion:
Okay…so this explains why infants are at greatest risk of infection from meningococcal disease, and it also explains why the rates in infants were so high between 1991 and 2002. The complement system is activated by the immune system’s response to antigens. Different parts of the system are activated by different antigens (viruses, bacteria, etc.). The complement proteins themselves are dependent on enzymatic processes in order to work properly, and they also depend on the stability of the permeability of the cell membranes.
One of the risk factors listed by the CDC is “antecedent viral infection” – meaning a viral infection that happened prior to exposure to meningococcal bacteria. This makes sense because if you have been exposed to a virus, C1 and C4 will be activated to fight the virus. Because of the way the system works, activation of the earlier complements disrupts the stability of the system and would be expected to cause a depletion in the successive complements (which are necessary to fight bacterial infections) – think of the see-saw metaphor, when one goes up another comes down.
Administration of the hepatitis B vaccine at birth was initiated in 1988-89 and by 1990 it was widespread. Hepatitis B is a virus.
Another risk factor mentioned by the CDC is “active or passive smoking.” Why would smoking cause an increase in the risk for meningococcal infection? Because of exposure to toxins that deplete antioxidants and minerals, especially vitamin C (necessary for glutathione), magnesium and zinc (necessary for integrity of cellular membranes, including the blood-brain barrier). When zinc is depleted or out of balance with calcium and magnesium, the blood brain barrier becomes more permeable (bigger holes), which increases the efficiency of passage of viruses (like measles and viruses in the herpes family) into the central nervous system. Cigarette smoke is ONE source of toxins that deplete minerals and glutathione. Mercury is another, and mercury accomplishes the disruption of minerals and antioxidants at a much greater level than cigarette smoke.
The childhood vaccination schedule was greatly increased throughout the 1990s and included multiple vaccines that contained toxic levels of mercury in the form of Thimerosal.
Now… go back to the definition of the complement system and notice the importance of enzymes and enzymatic cleavage. Enzymes are catalysts. They make things happen. When enzymes are messed up, things do not happen the way they are supposed to. Mercury (and other toxins, including aluminum and lead) damages enzymatic processes throughout the body. This is why heavy metals are SO dangerous and why they cause SO MANY different manifestations of illness; they destroy the enzymatic processes in the body, so NOTHING works the way it’s supposed to.
Questions:
1. Why would adolescents now be at increased risk of meningococcal infection?
Answer: In the past several years adolescents have been the target of increased vaccination, including flu vaccines that contain mercury, and Tdap and pneumococcal vaccines that contain aluminum and formaldehyde.
2. Why would college students (particularly college freshmen) be at increased risk of meningococcal infection?
Answer: Colleges and Universities have policies that require incoming freshmen to prove “up-to-date” vaccination before being allowed to register for classes. Freshmen are therefore vaccinated at higher rates than upper classmen. There is a very high risk for over-vaccination in college freshmen, particularly among those who may not have ready access to their childhood medical records and who, thinking there is no risk from vaccines, opt to simply get more shots rather than going through the steps necessary to prove they are “up-to-date” or have established immunity. Freshmen living in dormitories are more likely to be exposed to other freshmen whose immune systems are also damaged from mass over-vaccination, resulting in increased infections of all kinds.
3. How can you, as a parent, best protect your child from meningococcal infection?
Answer: Improve your child’s immune system by providing a healthy diet of whole foods that are rich in nutrients. Give supplements that are high in antioxidants, balanced B-vitamins (with the active form of folate – not folic acid), minerals and essential fatty acids. Give extra vitamin D3 during “cold and flu season.” Heal the gut if your child has gastrointestinal problems. Stress the importance of getting enough sleep, sunshine, and fresh air. Help your child learn to relax. And just say NO to vaccines that damage your child’s innate immune system.
Read the Vaccine Manufacturer’s Inserts:
Back to VAERS and the results of this morning’s queries…
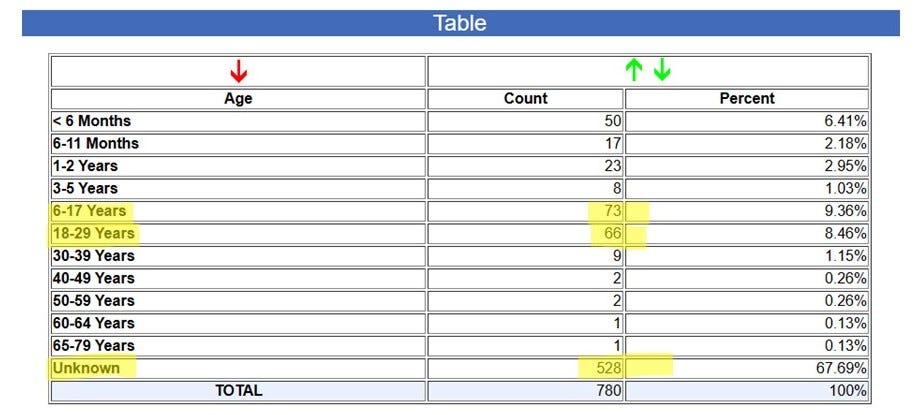
Of the 780 cases of meningococcal vaccine-induced meningococcal infection, in a large percent of cases, the age of the person was unknown. Of those for whom age was known, the largest percentage of cases occurred in adolescents and young adults.
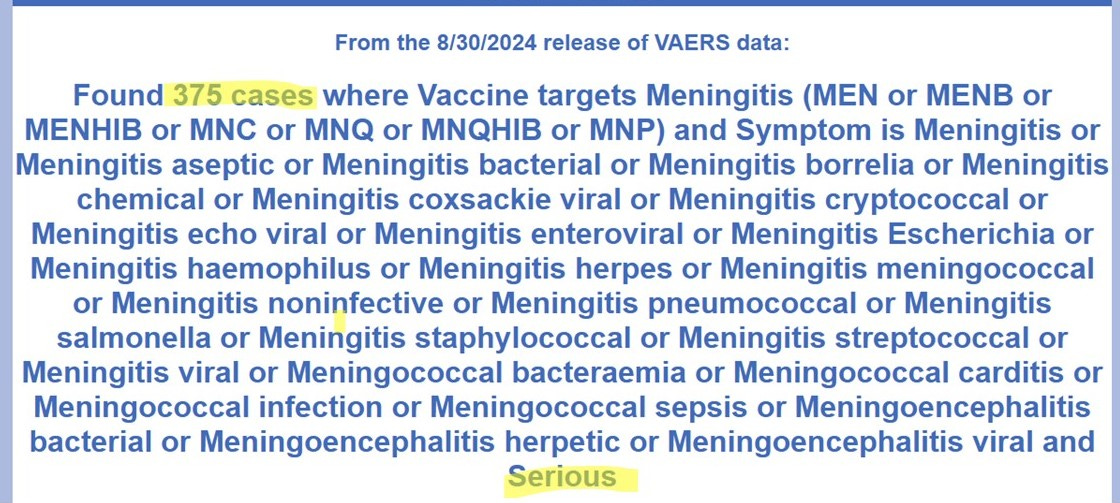
There were 375 cases that were deemed “serious.”
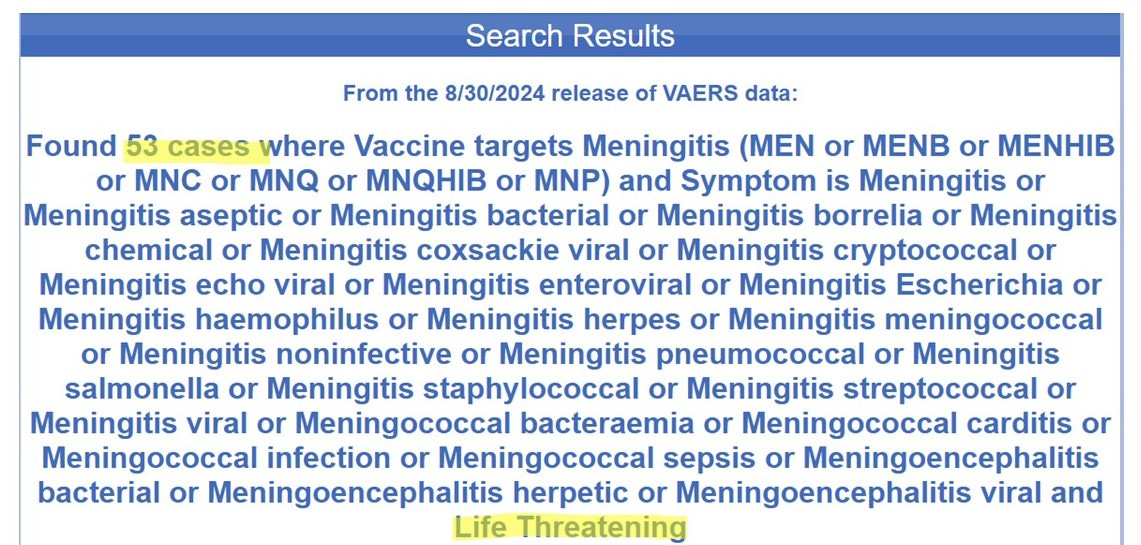
There were 53 “Life Threatening” reactions reported.
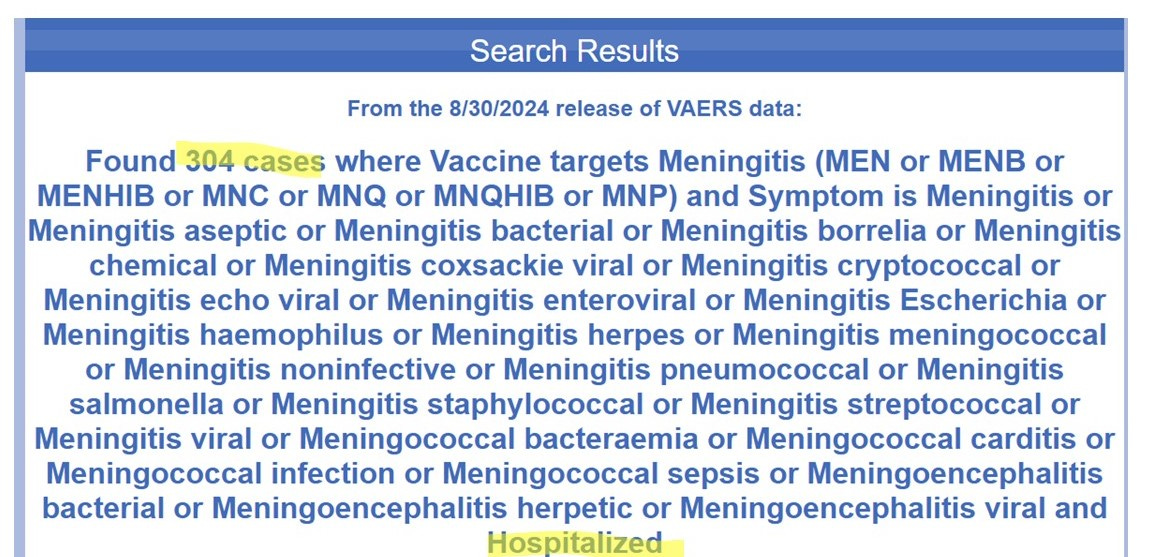
Of the 780 cases of meningococcal vaccine-induced meningococcal infection, 304 patients were hospitalized.
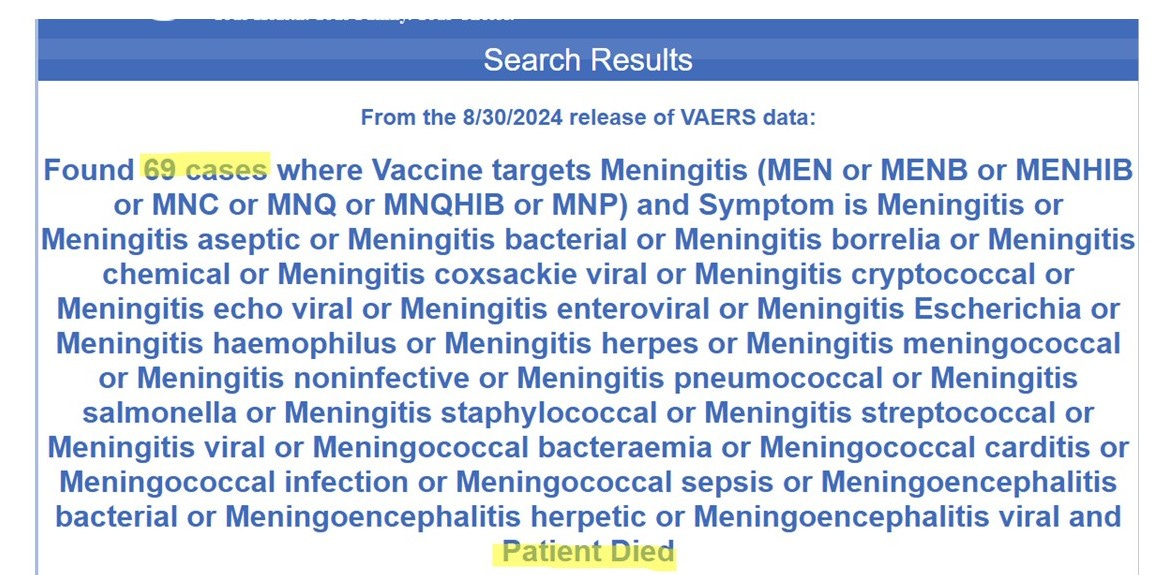
Of the 780 cases of meningococcal vaccine-induced meningococcal infection, 69 patients died.
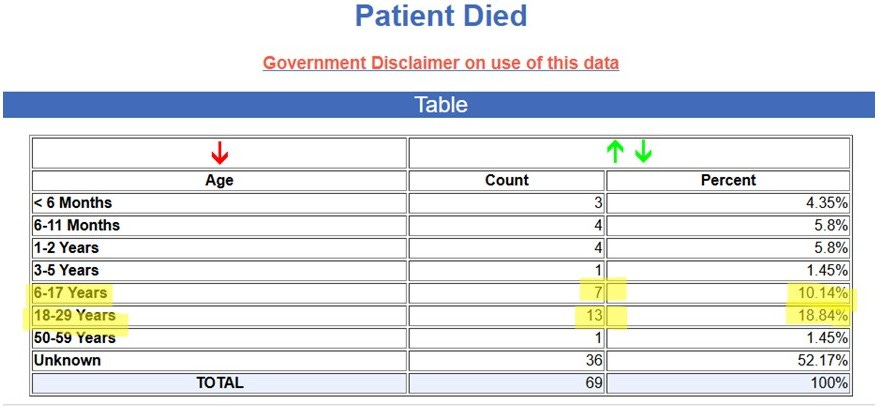
Of the 69 deaths reported to VAERS from meningococcal vaccine-induced meningococcal infection, 20 deaths were in adolescents and young adults. Here is what happened to them:
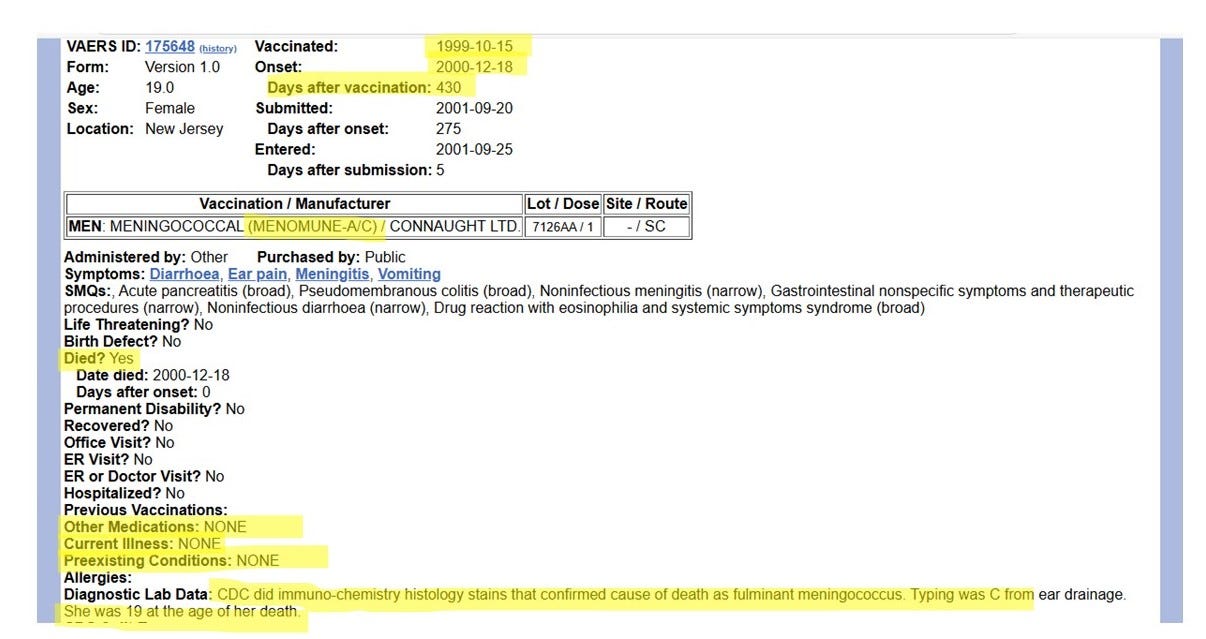
Case 1: A 19-year-old female from New Jersey, vaccinated with Menomune A/C, developed meningococcal infection (Type C, the same she was vaccinated with) and died from that infection. Her death occurred 430 days after she was vaccinated. She had no known preexisting health conditions.
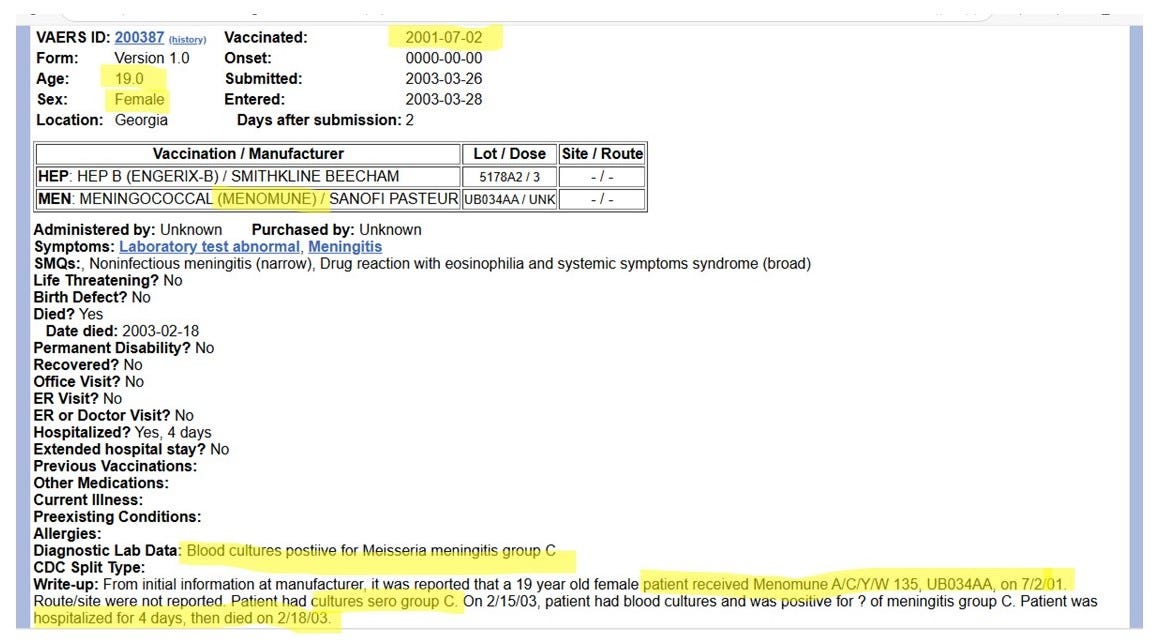
Case 2: A 19-year-old female vaccinated with Menomune A,C,Y,W on July 2, 2001 died nearly two years later on February 18, 2003 after developing a fatal meningococcal Type C infection (same type she was vaccinated with).
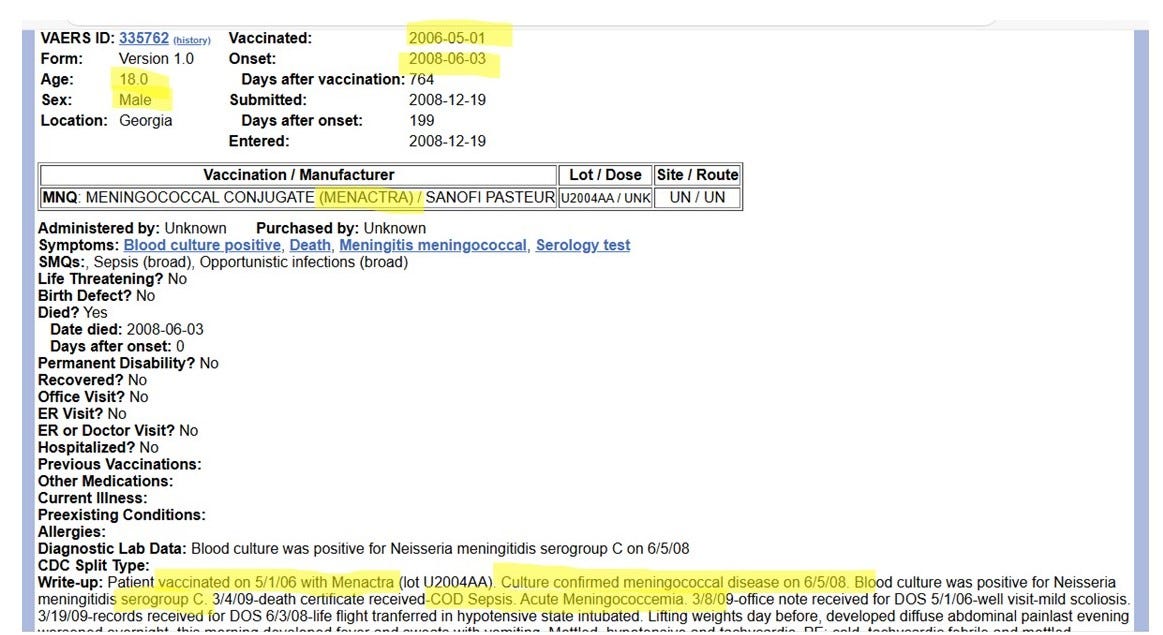
Case 3: An 18-year-old male was vaccinated on May 1, 2006 with Menactra (A,C,W,Y). He died from meningococcal infection Type C (the same type he was vaccinated with) on June 3, 2008. His death occurred slightly more than two years after vaccination.
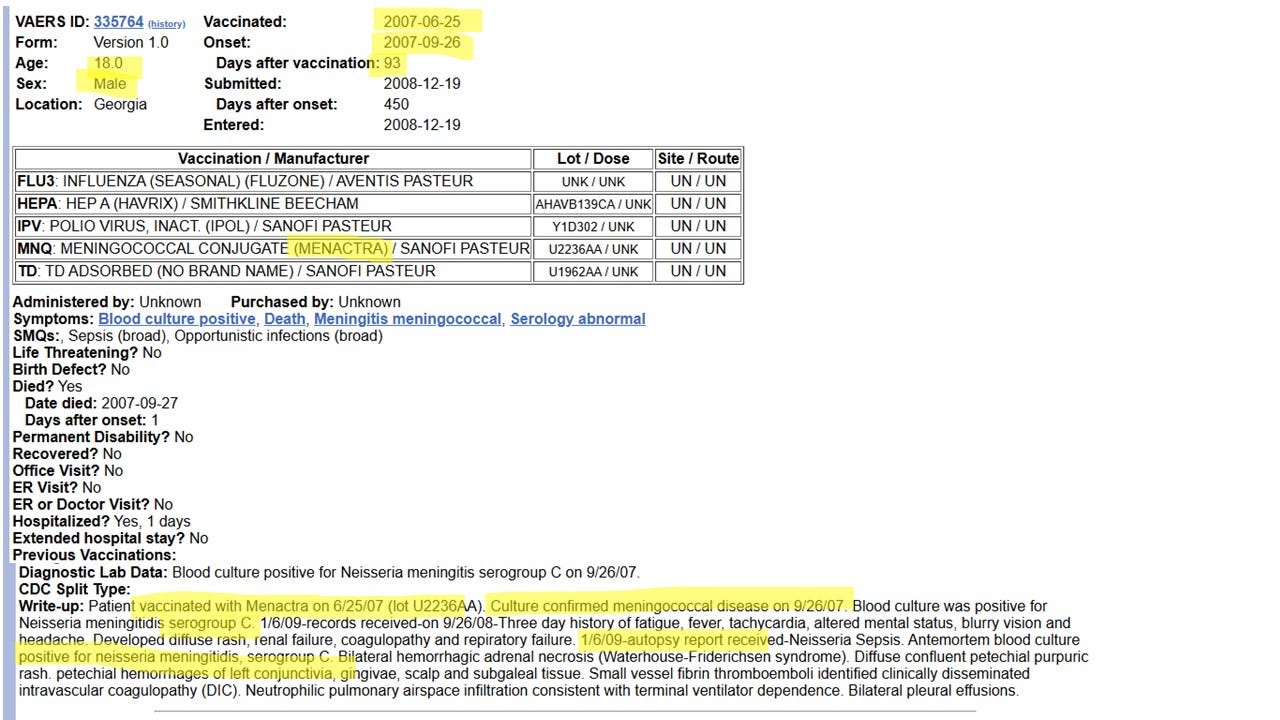
Case 4: 18-year-old male, vaccinated with Menactra (A,C,W,Y) on June 25, 2007, died three months later on September 27, 2007 from meningococcal infection Type C (same type he was vaccinated with).
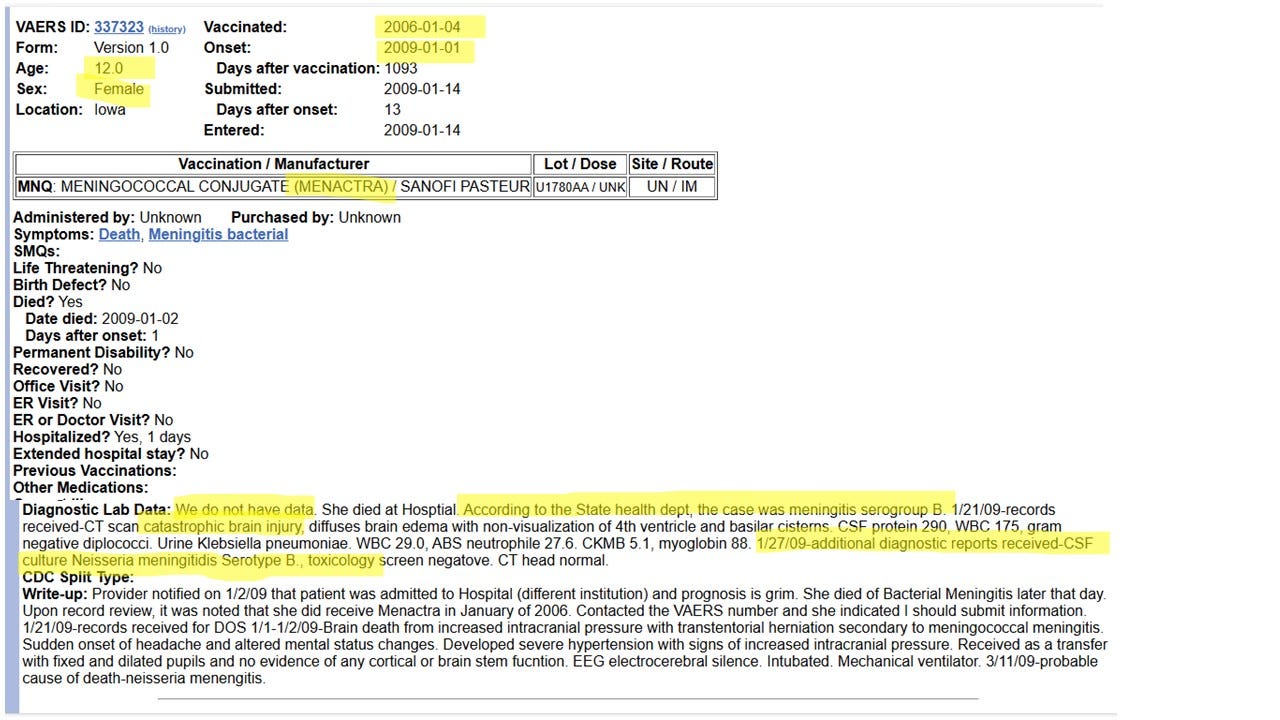
Case 5: A 12-year-old-female vaccinated January 4, 2006 with Menactra (A,C,W,Y) died three years later on January 2, 2009 from catastrophic brain injury caused by bacterial meningococcal infection (strain B).
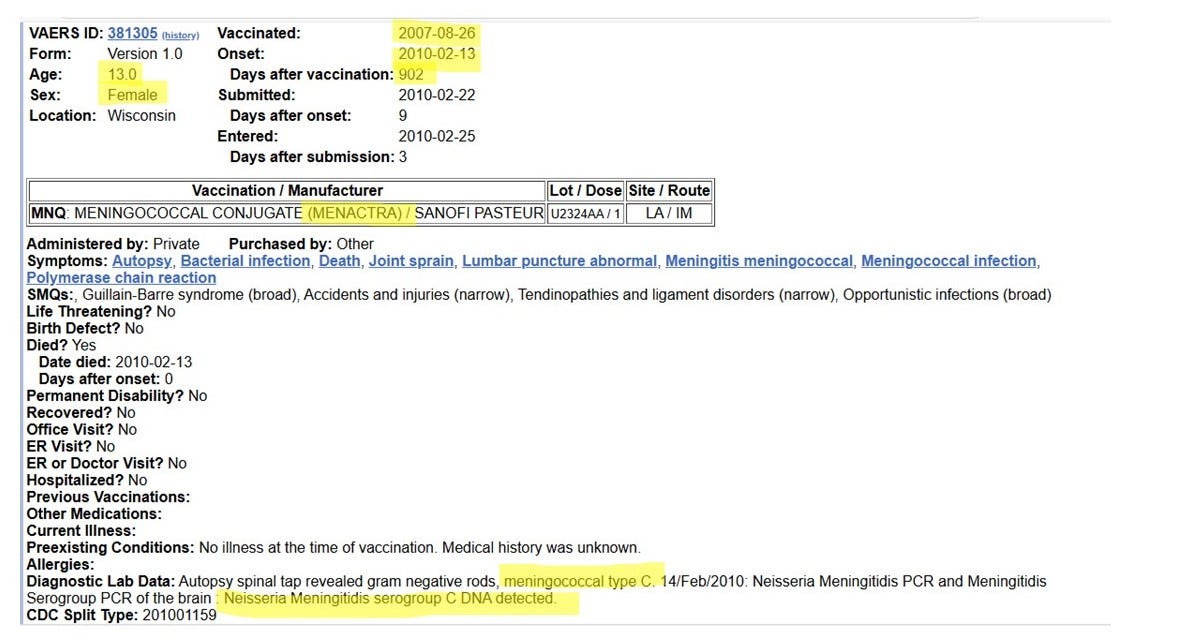
Case 6: A 13-year-old-female, vaccinated on August 26, 2007 with Menactra (A,C,W,Y), and died two and a half years later on February 2, 2010. Cause of death was meningococcal type C - same type she was vaccinated with.
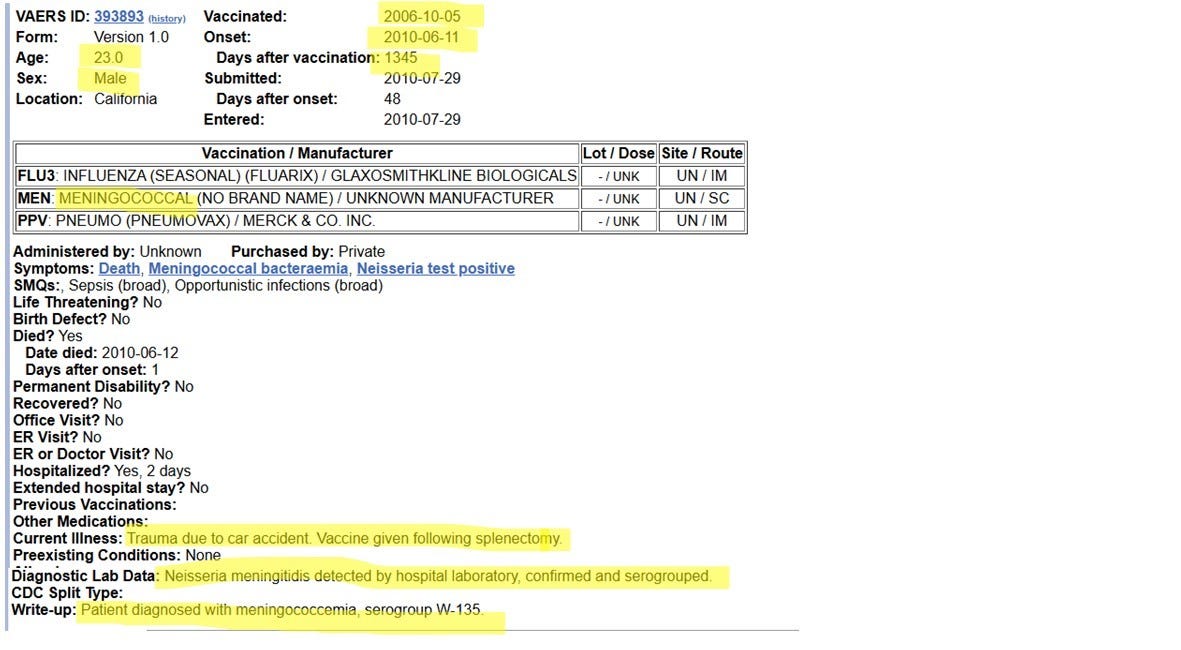
Case 7: A 23-year-old-male vaccinated on October 5, 2006 with unknown meningococcal vaccine (A,C,W,Y). The patient was hospitalized after a car accident and had his spleen removed, so they gave him the vaccine in the hospital. He died on June 12, 2010 from meningococcal infection type W - which was contained in the vaccine he received. (Note: We know it was A,C,W,Y vaccine because the meningococcal B vaccine was not licensed at that time.)
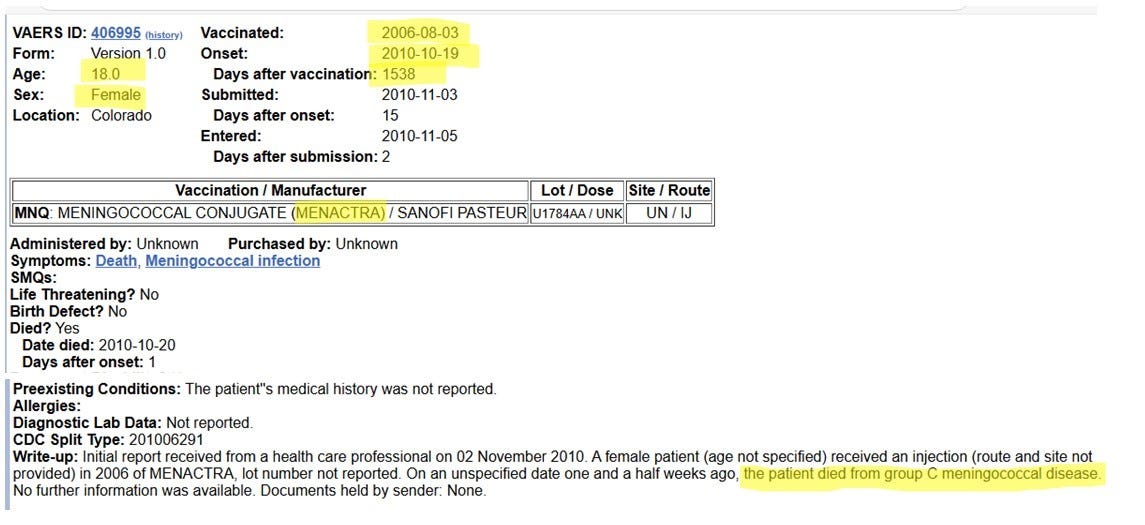
Case 8: An 18-year-old female, vaccinated August 3, 2006 with Menactra (A,C,W,Y). Died from group C meningococcal infection (which she was vaccinated with) on October 20, 2010 - four years after vaccination.
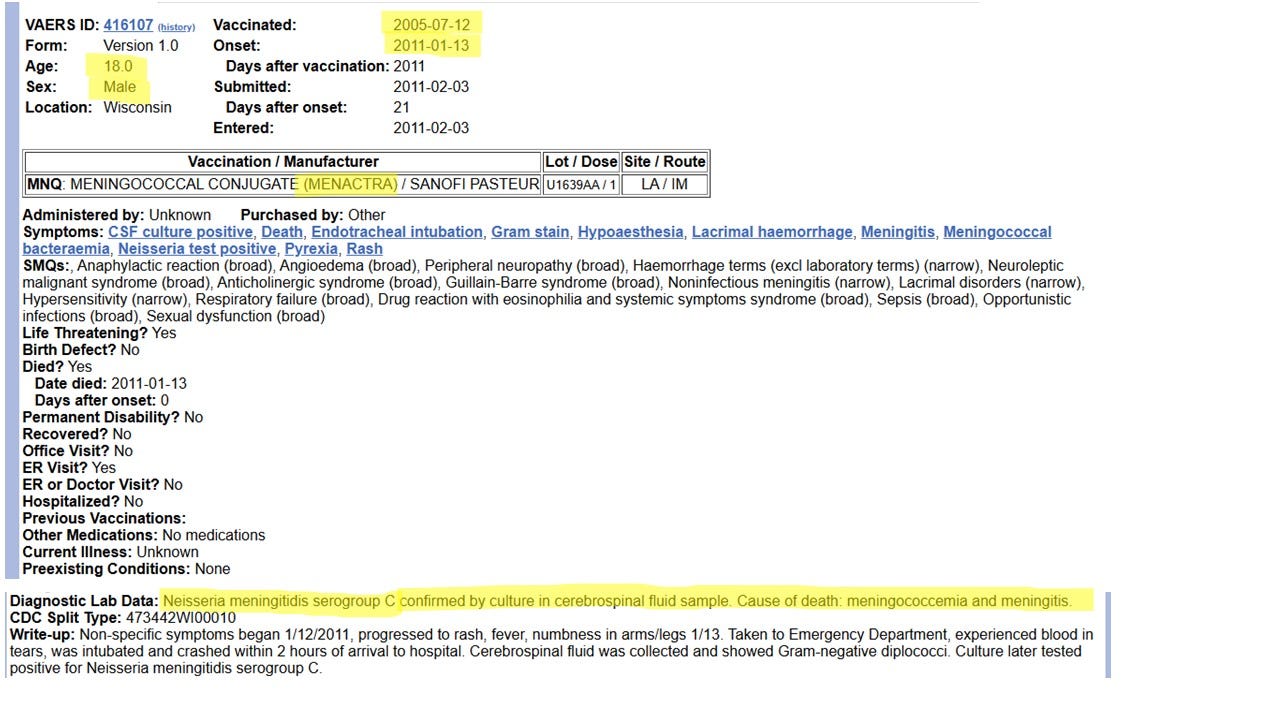
Case 9: 18-year-old male vaccinated July 12, 2005 with Menactra (A,C,W,Y). Died from meningococcal infection type C (same type he was vaccinated with) on January 13, 2011 - five and a half years after vaccination.
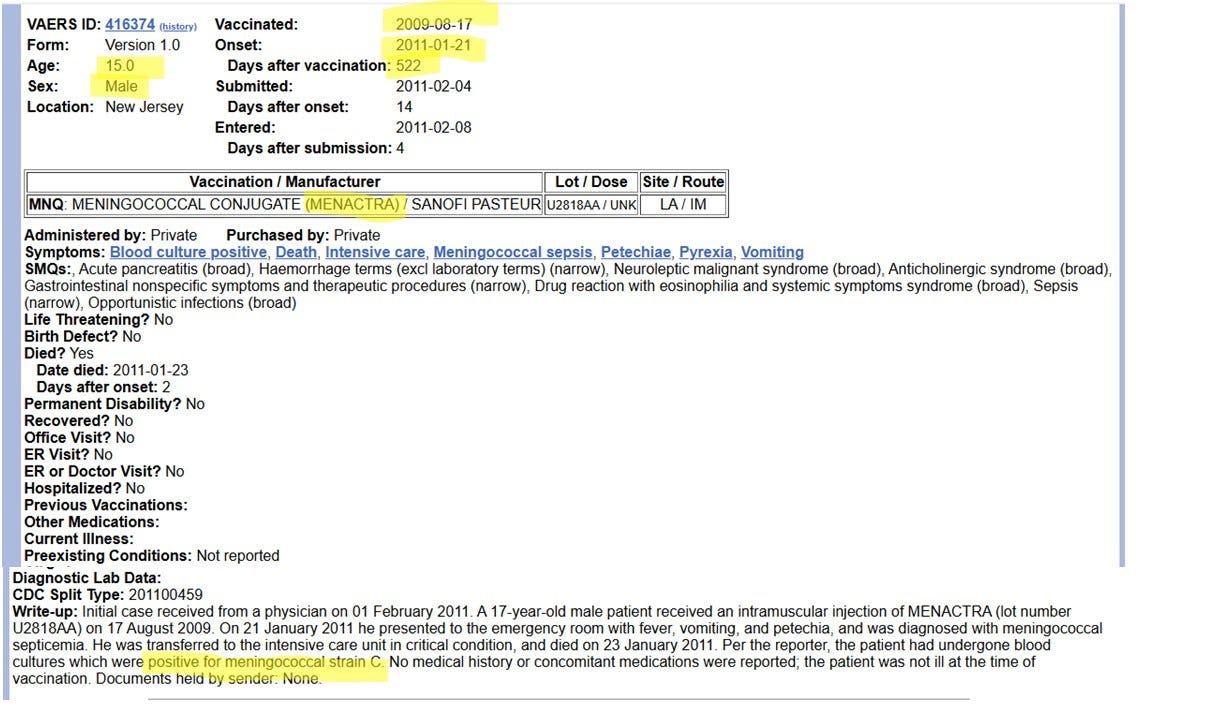
Case 10: A 15-year-old male vaccinated on June 17, 2009 with Menactra (A,C,W,Y). Died January 23, 2011 from meningococcal infection type C (same type he was vaccinated with).
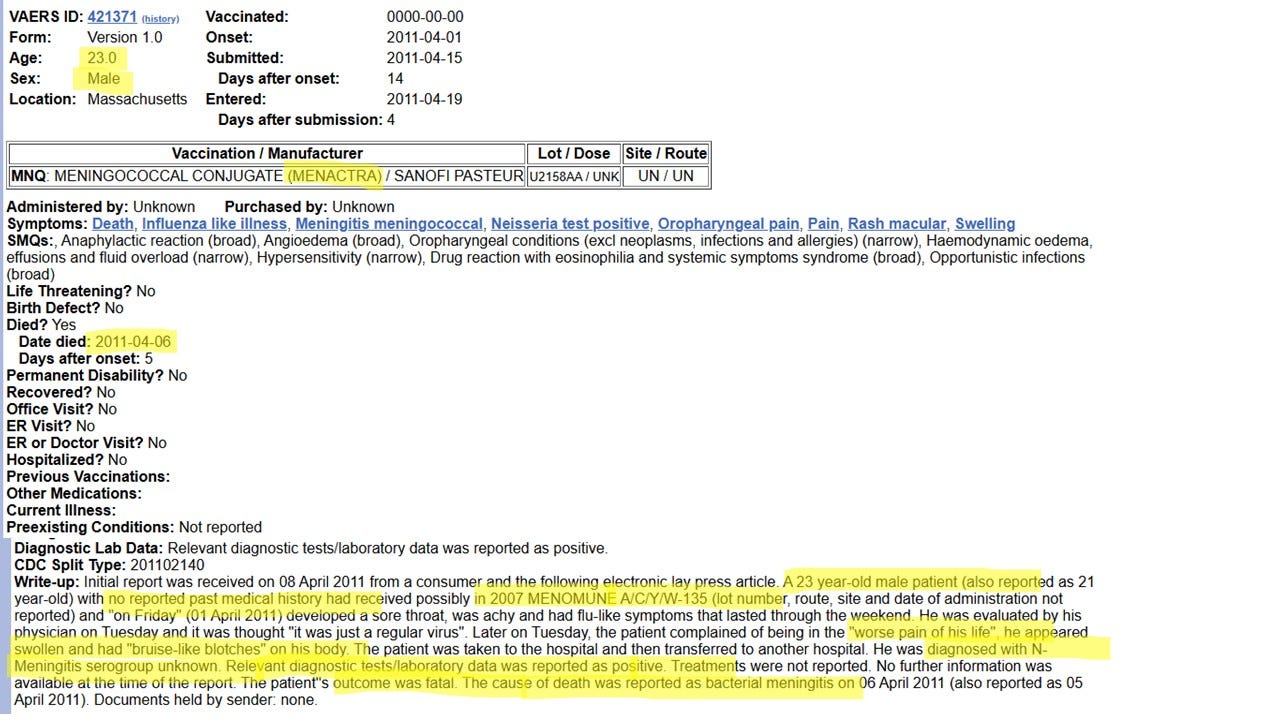
Case 11: A 23-year-old male, vaccinated with Menactra (A,C,W,Y) or Menomune (A,C,W,Y) around 2007, died from bacterial meningitis on April 6, 2011. Type unknown.
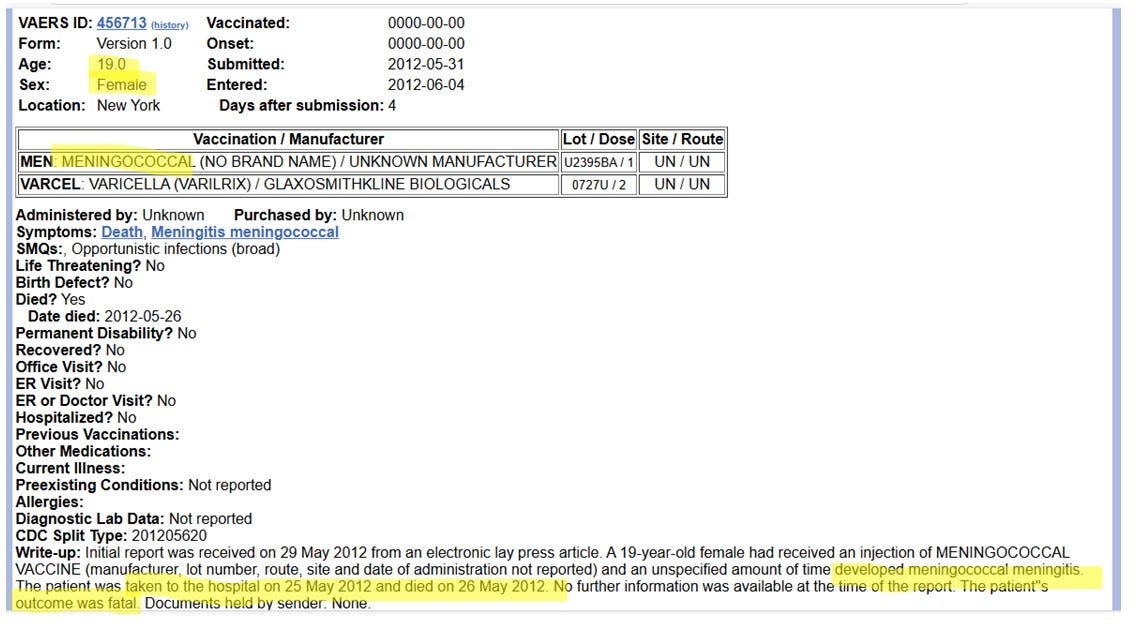
Case 12: A 19-year-old female vaccinated with unknown meningococcal vaccine (A,C,W,Y) died May 26, 2012 from meningococcal meningitis.
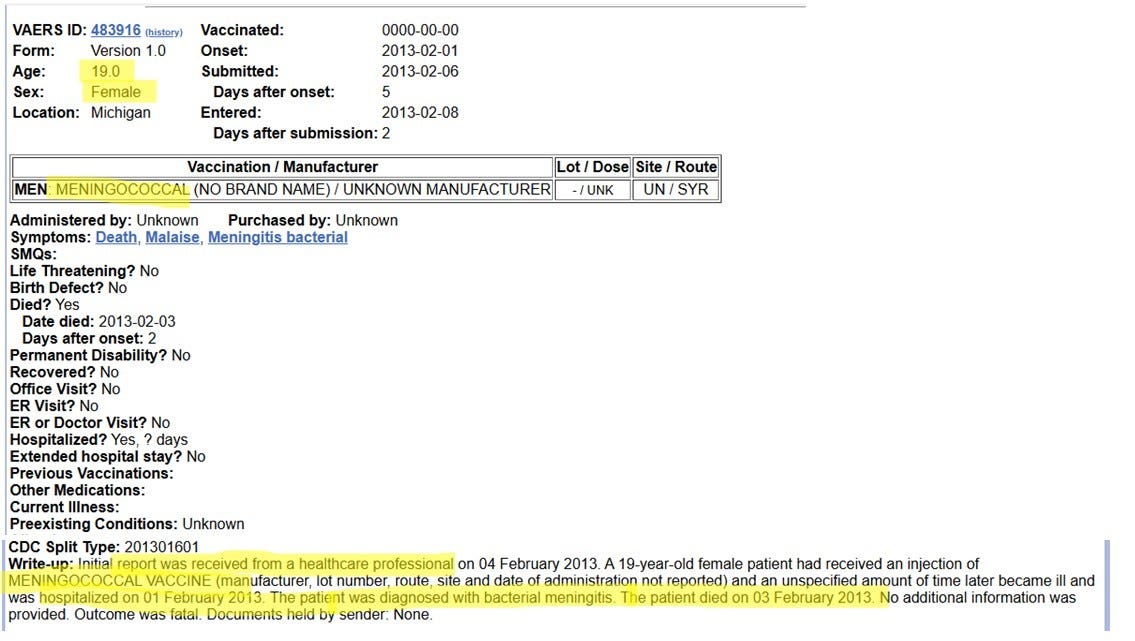
Case 13: 19-year-old female vaccinated with meningococcal vaccine (A,C,W,Y) died from bacterial meningitis on February 2, 2013.
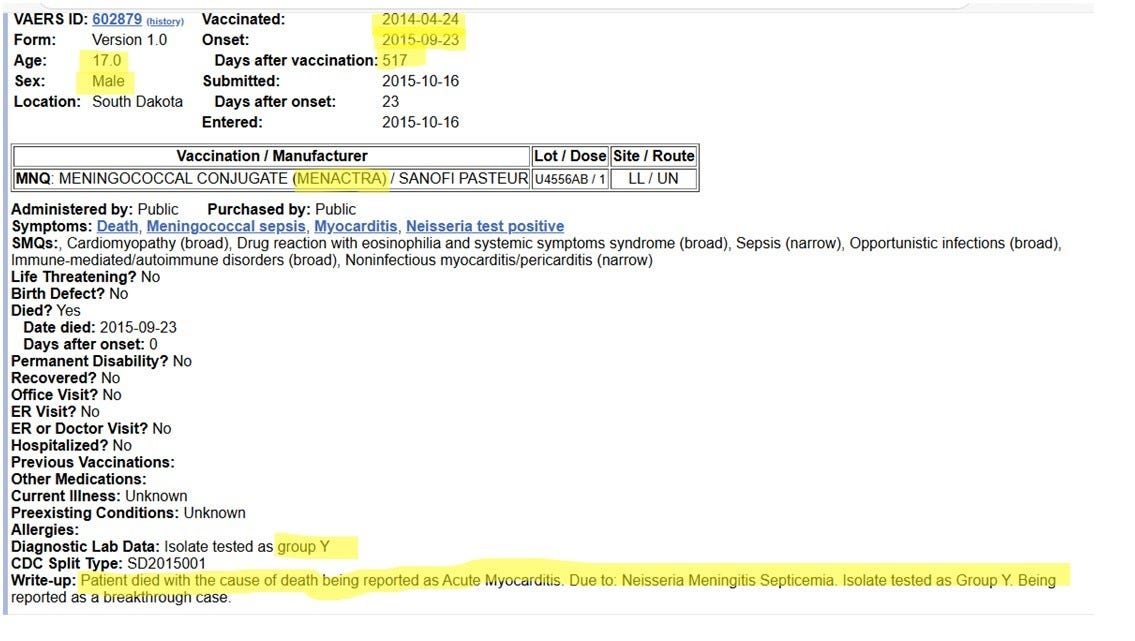
Case 14: 17-year-old male vaccinated with Menactra (A,C,W,Y) on April 24, 2014, died Septmber 23, 2015 from meningitis group Y (which he was vaccinated with).
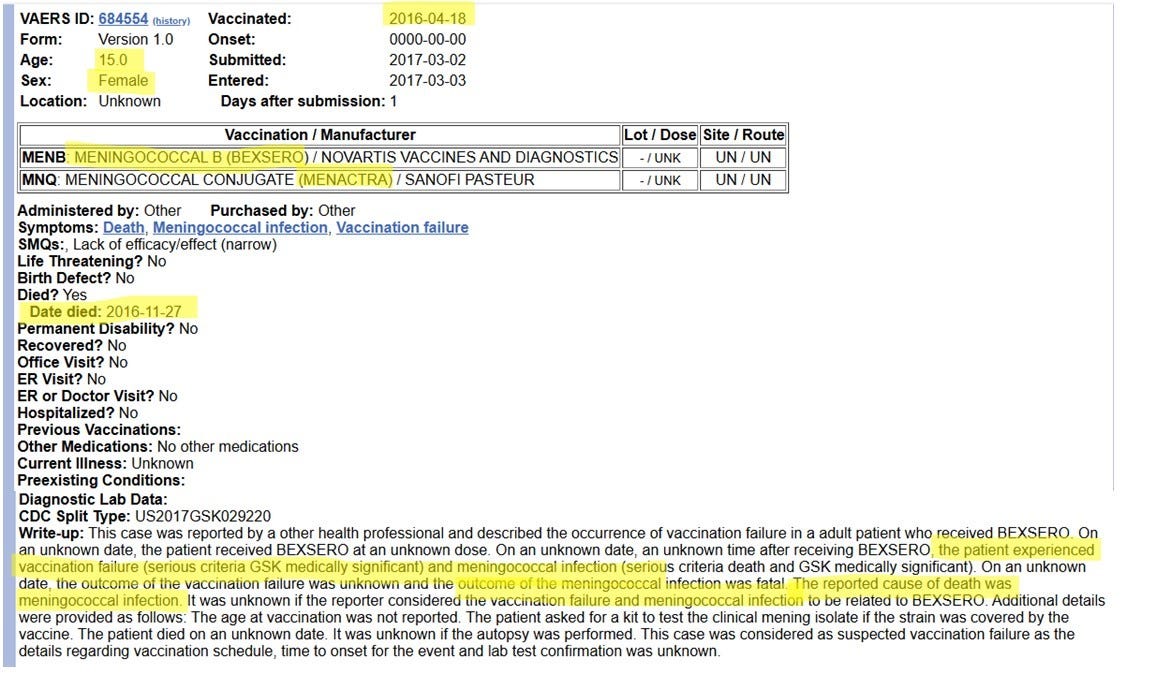
Case 15: A 15-year-old female vaccinated April 18, 2016 with Menactra (A,C,W,Y) and BEXSERO (B), died November 27, 2016 from meningococcal infection. Her death was deemed as being due to “vaccine failure.”
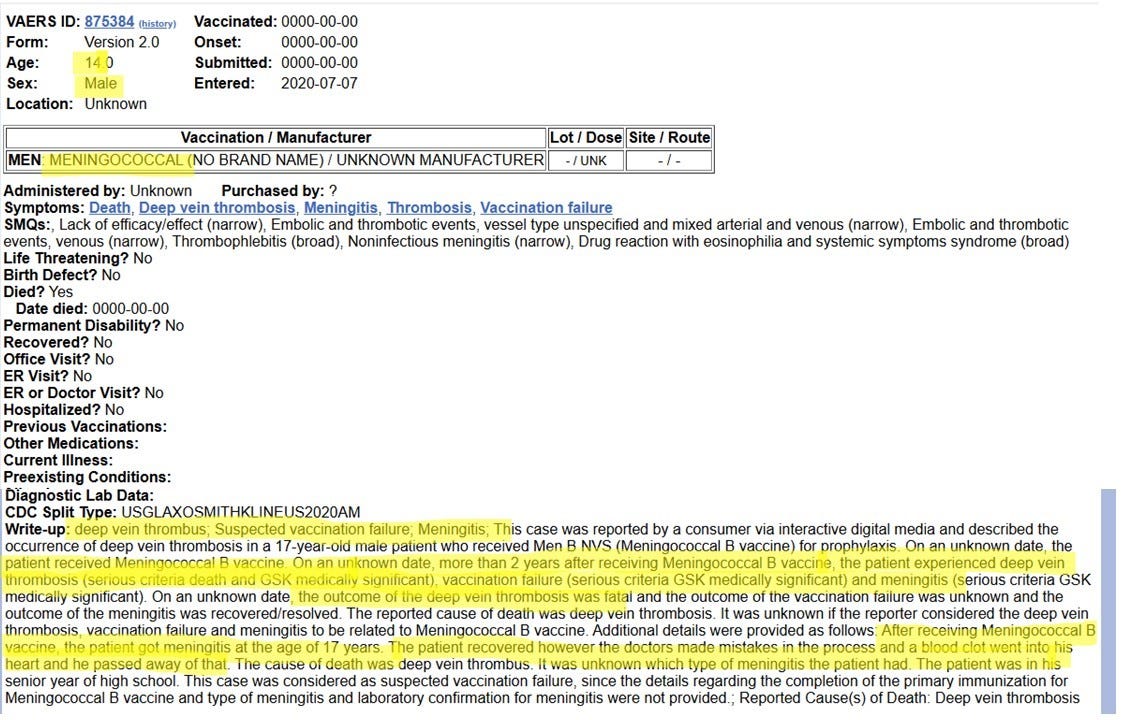
Case 16: This appears to be a case where a 14-year-old male was vaccinated with the meningococcal B vaccine and two years later developed meningococcal infection, with subsequent deep vein thrombosis, from which he died. His death was deemed as being due to “vaccine failure.”
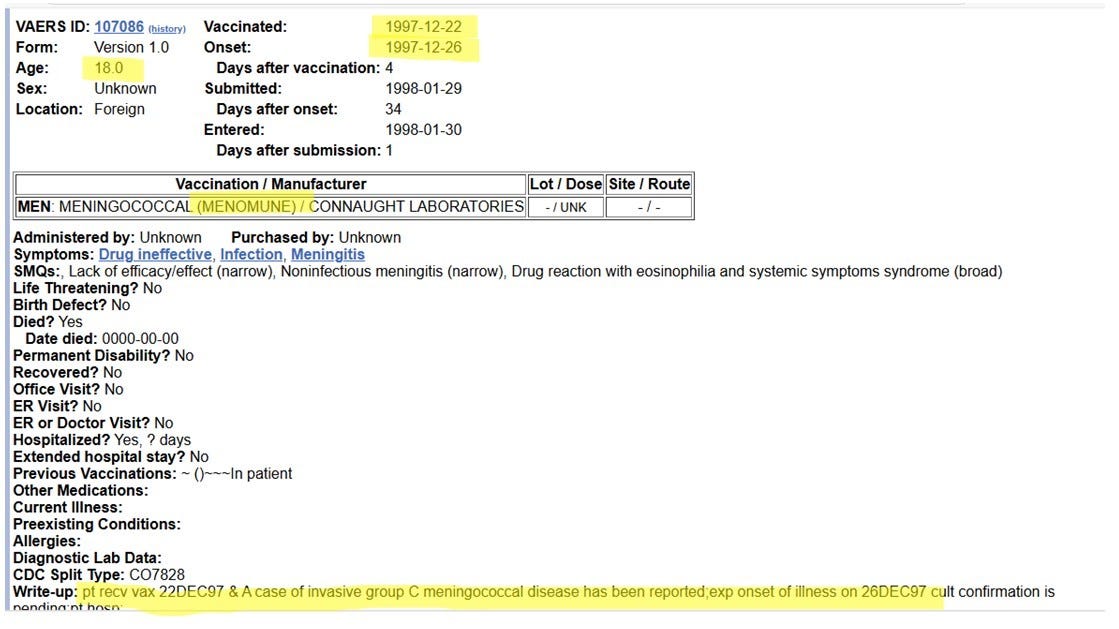
Case 17: An 18-year-old vaccinated with Menomune (A,C,W,Y) on December 22, 1997 died four days later on December 26, 1997 from meningococcal infection group C (which he was vaccinated with). Note the symptoms are described as “lack of efficacy” and “noninfectious meningitis.” I would say that’s a bit more than “lack of efficacy.”
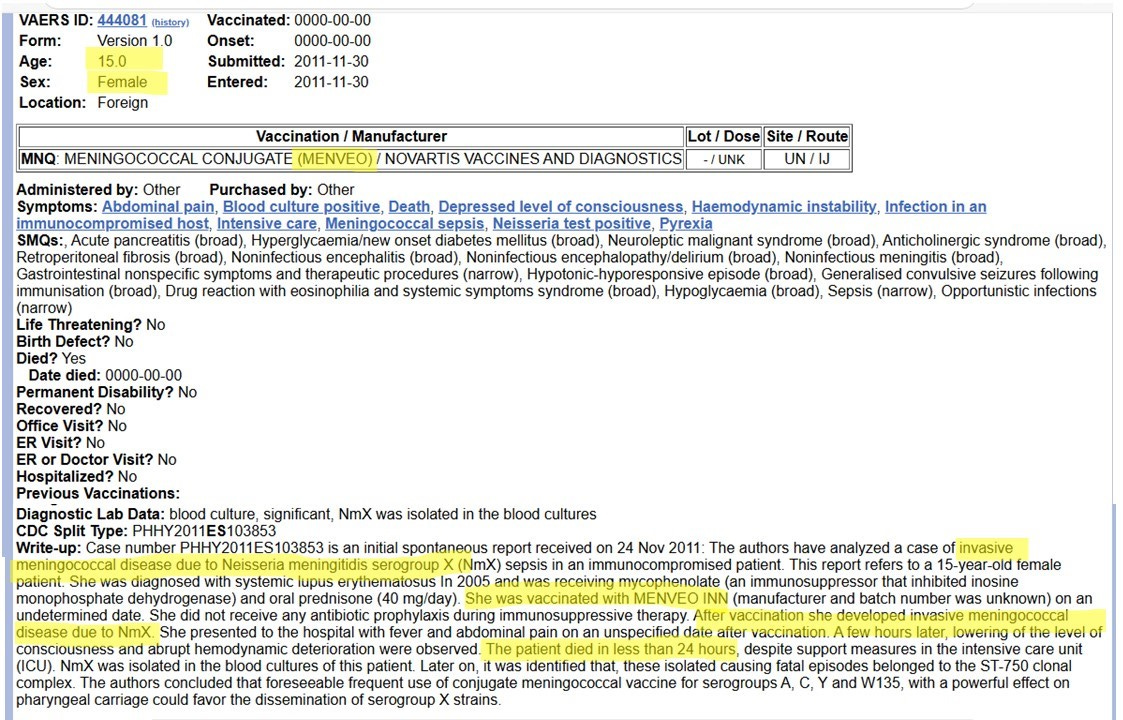
Case 18: A 15-year-old female vaccinated with Menveo (A,C,W,Y). “After vaccination she developed invasive meningococcal disease due to NmX.” She died in less than 24 hours.
Please note the last sentence in the above report: The authors concluded that foreseeable frequent use of conjugate meningococcal vaccine for serogroups A,C,Y and W135, with a powerful effect on pharyngeal carriage could favor the dissemination of serogroup X strains. What this means is that because the meningitis vaccines are “partial coverage” vaccines - they do not cover all strains that cause meningococcal infection, they cause an increase in the risk of developing other meningococcal infections that are not covered in the vaccine.
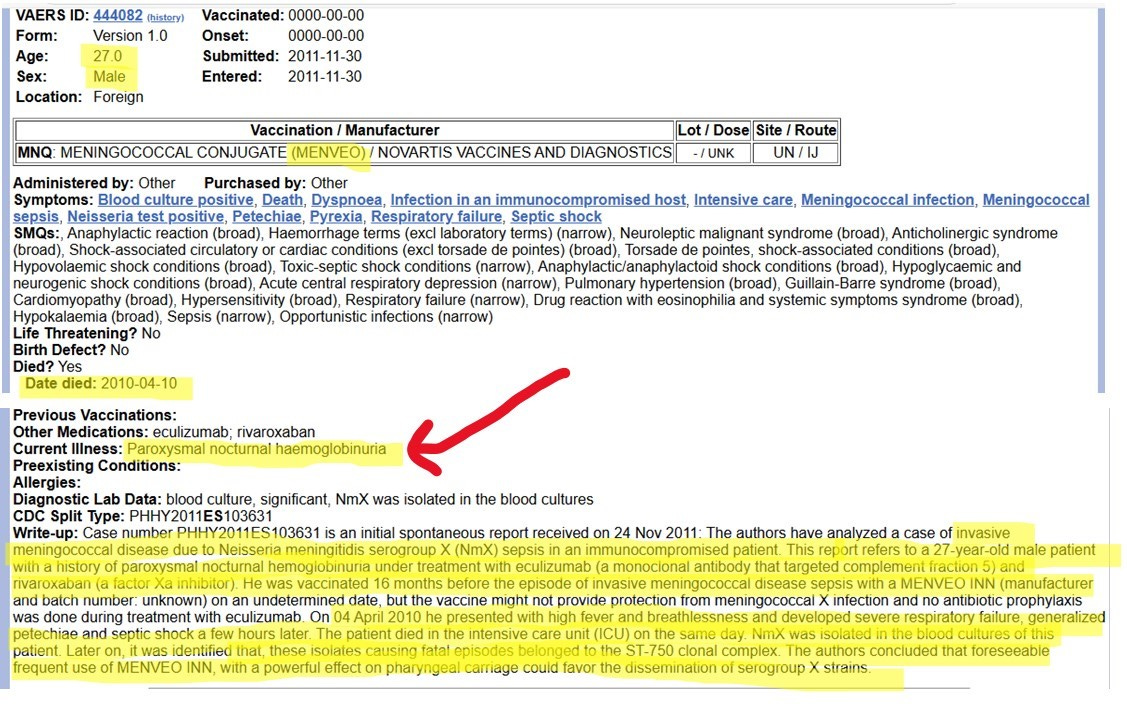
Case 19: A 27-year-old male vaccinated with Menveo (A,C,W,Y) developed “invasive meningococcal disease due to Neisseria meningitidis serogroup X (NmX) sepsis in an immunocompromised patient. This report refers to a 27-year-old male patient with a history of paroxysmal nocturnal hemoglobulinuria…” (Same diagnosis as Alexis Lorenze)
There it is again… The last sentence: “The authors concluded that foreseeable frequent use of MENVEO INN, with a powerful effect on pharyngeal carriage could favor the dissemination of serogroup X strains.”
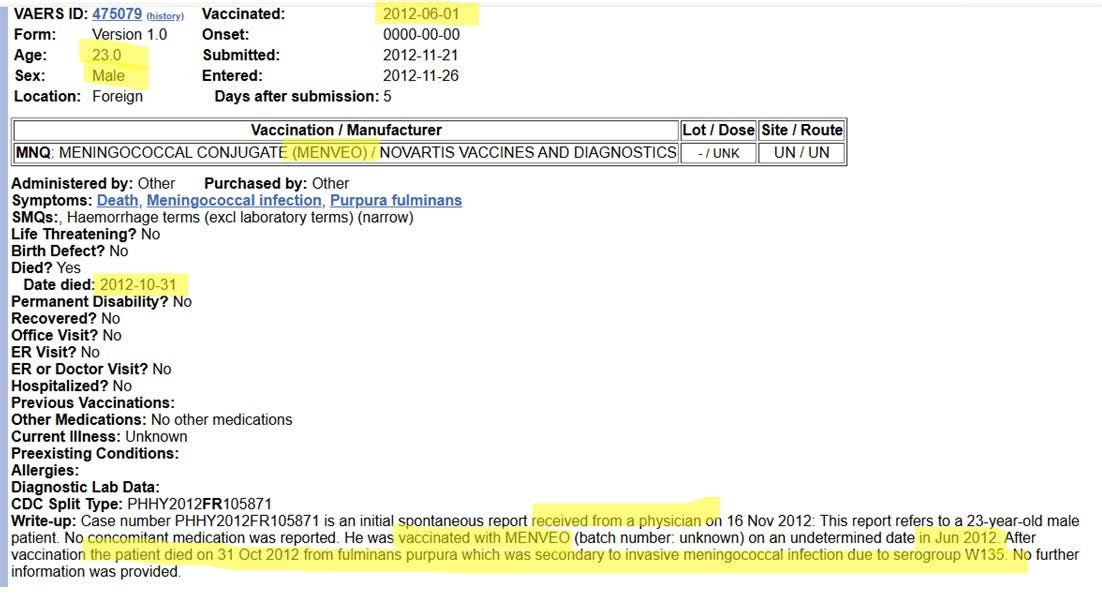
Case 20: A 23-year-old male vaccinated with Menveo (A,C,W,Y) in June of 2012. He died on October 31, 2012 “from fulminans purpura which was secondary to invasive meningococcal infection due to serogroup W135 (which he was vaccinated with).”
FYI… fulminans purpura is the purple patches on the skin… like Alexis Lorenze is experiencing.
From these twenty reports of deaths in adolescents and young adults from meningococcal vaccine-induced meningococcal infection, we can glean the following:
The vaccine does not prevent the development of meningococcal disease. Those who are vaccinated can and do develop severe, fatal meningococcal infections, and those infections can be from the same serotypes the vaccines contain.
As a partial coverage vaccine, the meningococcal vaccine can increase the risk of developing severe, fatal meningococcal infection from serotypes that are not covered in the vaccine.
The development of severe, fatal meningococcal infection after vaccination may occur quickly (within days to weeks) or it may occur years after vaccination.
Given that death from meningococcal infection is extremely rare in the United States, occurring in approximately 1.5 out of 10 million people each year (per the CDC’s numbers), and given that the vaccine itself can increase the risk of serious infection and death, why would you, as a parent, subject your child to this vaccination? Why would any parent do so? The answer is fear. Fear perpetuated by the CDC, and by groups such as the Voices of Meningitis. Fear perpetuated by doctors and nurses, who are “educated” by the CDC, and whose “education” regarding vaccines is limited to the following three bullet points:
“Vaccines are the greatest invention in modern medicine. Vaccines save lives. Vaccines never harm, and in the rare occasions when it looks like they do, it’s not the vaccine’s fault - there is something wrong with the child/person... It’s coincidence.”
“Learn the CDC Childhood Schedule. Never deviate from THE SCHEDULE.”
“When parents question, respond with bullying, threats, and intimidation. Do anything necessary to obtain compliance.”
Please read the following commentary by Robert F. Kennedy, regarding his concerns about New York State (and others) mandating the meningitis vaccine for school attendance. As anyone who takes the time to do the math can see, the motivation for the mandates can only be financial…
Reasons for proposed meningitis vaccine don’t add up
Commentary by Robert F. Kennedy, Jr.
June 9, 2015
“New York lawmakers should do some simple math before voting on the proposed bills to compel all New York school children to receive the meningococcal meningitis vaccine.
“Because immunization from the meningitis vaccine wanes rapidly, the proposed law (A791C and S4324A) will force New York schoolchildren to take the current meningococcal vaccines twice; first in the seventh grade and again in the 12th grade. Each year, about 400,000 seventh- and 12th-graders would be vaccinated or banned from school.
“Meningococcal meningitis is exceedingly rare. There were only about 390 cases in the United States last year, according to the Centers for Disease Control and Prevention, and the rates were dropping before the vaccines came into use. In a population of 319 million, that is 1 case in 817,949 people. Further, most cases — 98.5 percent — are sporadic, not part of an outbreak.
“CDC has licensed three vaccines for the A, C, Y and W135 strains of meningitis: Menactra, Menveo, and Menomune, which still contains massive mercury concentrations in multidose vials. These vaccines are only effective in providing immunity in about 85 percent of inoculated children. Thirty percent of the meningitis cases are the B strain, against which these vaccines are completely ineffective.
“According to their package inserts, the current vaccines have "serious adverse event" rates of 1 percent for Menactra and Menveo and 1.3 percent for Menomune with its hefty mercury load. According to the CDC Pink Book, 0.3 percent of those with "serious adverse events" from meningitis vaccines will die.
“So here is the math calculation that thoughtful New York lawmakers must mull over: By inoculating 400,000 New York schoolchildren, they may spare four children from contracting meningococcal meningitis — at a cost of 4,000 seriously sickened children and 12 dead.
“That's not the worst part. The FDA recently approved two B strain meningococcal vaccines, Trumenbu and Bexsero. Vaccine makers are pushing CDC to add them to the recommended schedule. Critics have faulted the expedited safety and efficacy testing for the new B strain vaccines, citing glaring lapses in safety protocols. Neither vaccine has been tested for carcinogenicity, mutagenicity or effects on male fertility. The B vaccines product inserts indicate grim predictions; 2 percent, or 8,000 New York students, sickened with serious adverse events and 25 dead, according to the CDC Pink Book.
“There are budgetary costs as well. At an average total cost of about $150 per shot, there is huge corporate incentive to get these vaccines mandated. Nationwide, with about 4 million children in each birth cohort, the old meningitis vaccines alone are worth between $600 million and $1.2 billion annually to big pharmaceutical companies.
“For those with private insurance, premiums will increase. For those without insurance, the federally funded "Vaccines for Children" program will pay. This CDC entitlement program, with a current budget of over $4 billion, was originally intended to ensure that low-income kids in California received the measles vaccine. It has since mushroomed into a cash cow for any vaccine added to the recommended schedule — regardless of the communicability of the disease or cost-effectiveness of the particular vaccine.
“It gets worse. Language in the Senate and Assembly bills automatically mandate meningococcal B vaccines once CDC recommends them. Administration of Bexsero will cost $320 per student, according to the CDC vaccine price list — or $128 million annually. Adding this to the cost New Yorkers will pay for the old vaccines — $52 million annually — the total cost of this legislation will be $180 million every year.
“The costs of this bill, in both dollars and children's lives, could make sense only to coldblooded bean counters at the companies marketing these vaccines and to the politicians who have pocketed those companies' political contributions. And pharma fingerprints are in other places than the generous checks they have given the bill's sponsors.
“The legislation is unusual in that it supersedes the traditional authority exercised by state Department of Health officials over the vaccine schedule for New York schoolchildren. The legislation's authors mean to transfer that authority to the CDC's vaccine division, which has been plagued by a series of recent scandals and four scathing federal investigations, criticizing the agency's shoddy science and its corrupt conflicts of interest with vaccine manufacturers.
“Before we relinquish our sovereignty, squander our treasury and sicken our children, we should do the math.”
More…

About a month ago, I was chatting with a group of moms about homeschooling regrets. We shared and encouraged each other. (It was not a totally dark conversation.) When they asked me, I shared that my biggest regret was vaccinating my kids - especially with aborted fetal tissue.
The discussion continued with others sharing their various regrets and lessons learned. Then one of my closer friends returned to the topic of vaccines. I could tell she had been mulling my statement. She is still new to ‘alternative’ healthcare and asked me what she should do about the M vax. She has a 17yo son and admitted that she is terrified because of the propaganda. At the time, I empathized with her fear and advised that she read the list of ingredients before deciding.
When I read this article the other day, I immediately shared it with her. She texted me back, very appreciative for all the well-researched information.
So thank you for taking the time to research these things so thoroughly, explain them so clearly, and share them so freely. Because of you, I am MUCH better equipped to warn and encourage other moms.
I pray that God will bless you and your family with overwhelming joy, strength, protection, and provision. May He continue to give you insight and wisdom.
Marcella...this is a huge amount of info...thank you for giving your time to put it all together. You are a blessing