


Immune Deficiency and MMR - Who should NOT get a measles, mumps, rubella vaccine?
Assessment of the immune system is paramount before receipt of live viral vaccines.

You know how every time there is an “outbreak” of measles, the media and doctors talk about “the responsibility of those who CAN be vaccinated to do so, in order to protect those who CAN’T be vaccinated?” We usually hear about the immune compromised, those with autoimmune conditions, and people undergoing treatment for cancer, whose immune systems are significantly depressed. The message is, if you are healthy, you owe it to society to take the needle. It’s the weaponization of compassion.
I have never really looked at what the CDC or Merck (maker of MMR vaccine used in the U.S.) have to say about people who should NOT get the vaccine. As I was thinking about this, I started thinking about just how many children in the United States have significant immune system problems. A study published in 2011 found that 54% of American children have been diagnosed with at least one chronic illness. Many of those chronic illnesses are the manifestations of immune systems that have gone awry.
From the study:
An estimated 43% of US children (32 million) currently have at least 1 of 20 chronic health conditions assessed, increasing to 54.1% when overweight, obesity, or being at risk for developmental delays are included; 19.2% (14.2 million) have conditions resulting in a special health care need, a 1.6 point increase since 2003.
I have seen this study quoted in many places and have always just remembered that it was published in 2011. The thing is the authors used data collected in 2007. I know that the incidence of autism has increased exponentially since 2007. For those who may not know, autism is medical. Not mental. Children with autism often have very significant underlying medical conditions. They almost always have gastrointestinal issues. They frequently have strong histories indicative of immune system dysfunction, including recurrent infections (ears, throat, upper respiratory, gastrointestinal, etc…) which are treated with antibiotics and steroids. They also very frequently have strong family histories of autoimmune disorders. The incidence of autoimmune thyroiditis, rheumatoid arthritis, and Type I diabetes, psoriasis (source), ulcerative colitis, celiac disease (source), asthma and allergy (source) have been found to be significantly higher in parents of children diagnosed with regressive autism.
We observed nearly a 50% higher odds of being diagnosed with autism by age 10 years among children whose parents had any autoimmune disease. We used a large, representative sample with extensive, lengthy follow-up of individuals through the registry system. The overall association was observed for both mothers and fathers… (source).
The “official” numbers for U.S. children diagnosed with autism are released every few years by the CDC. They didn’t report in 2007, but in 2006, the “official number” for children with autism living in the United States was 1 in 110. In 2020, the “official number” was 1 in 36. And those numbers do not include any children under the age of twelve years. By the CDC’s own admission, the rate of autism, which manifests in children who have multiple signs of immune system dysregulation, has been increasing at a yearly rate of 13% since at least the year 2000.
This made me wonder if the rates of immune deficiency disorders are also increasing.
This study, which looked at the incidence of Primary Immune Deficiency Disorders used a national population-based database to estimate PIDD prevalence and hospitalizations. The researchers found:
Between 2001 and 2007, prevalence of any PIDD diagnosis increased from 38.9 to 50.5 per 100,000 (a 30% increase in six years) among privately insured and from 29.1 to 41.1 per 100,000 (a 41% increase in six years) among publicly insured persons.
So, we can probably safely assume that these trends are linked, and the number of children diagnosed with an immune deficiency disorder has increased considerably since 2007, just as has happened with autism.
More information from the study mentioned above:
When we stratified the CCE population by age, the older age groups (45–54, 55–64 years) had a higher prevalence for all PIDD diagnoses compared with the population aged 21 and younger. In the pediatric population, the average prevalence of any PIDD was highest in the 1–5 years age group (CCE 46 to 67 per 100,000; MC 29 to 42 per 100,000). For B cell defects, the average prevalence was highest in the 1–5 years range (MC 20 to 25 per 100,000) and increased across all years (p<0.0001). In the MC population, the highest prevalence for T cell defects was observed among children <1 year of age (MC 15.6 to 21.5 per 100,000) (source).
Okay. So, now we know that the rates of Primary Immune Deficiency Disorders are increasing in children. We also know that the rates of increase in the population aged 21 and younger are highest among children between birth and five years of age.
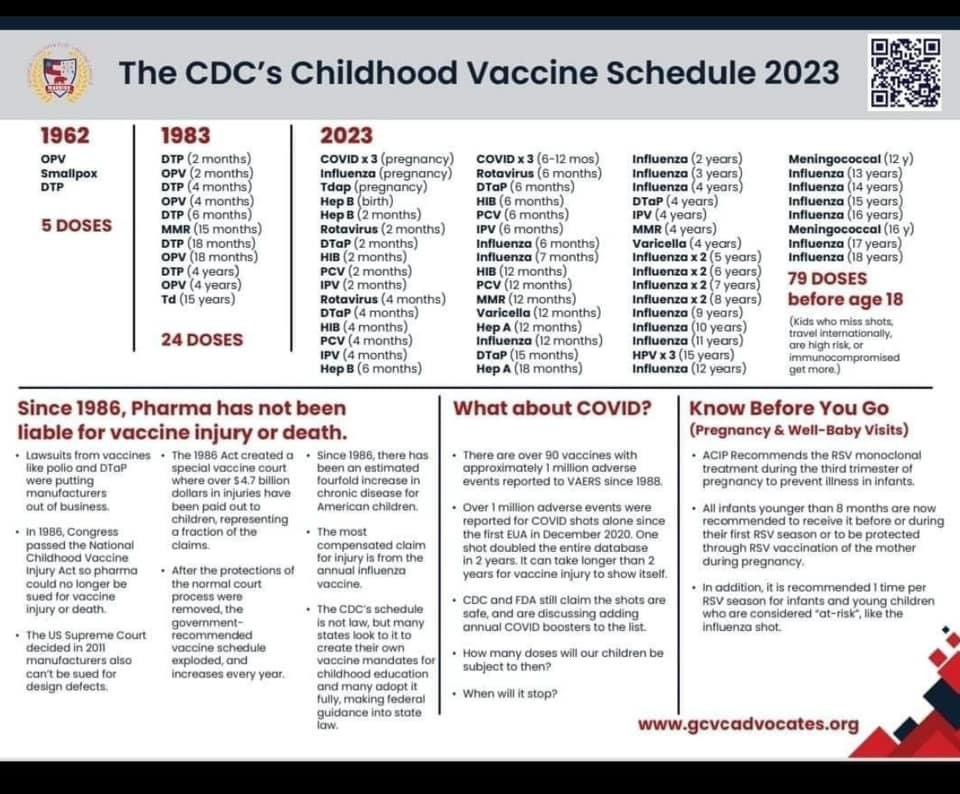
What happens to children between birth and five years of age? If they are vaccinated according to the CDC’s Childhood Schedule, they receive MANY vaccines. The number of vaccines given to infants and children between birth and age five has increased exponentially over the last several decades (since the passage of the 1986 law granting freedom from liability to the vaccine manufacturers and promoters). I found this graphic the other day on Facebook:
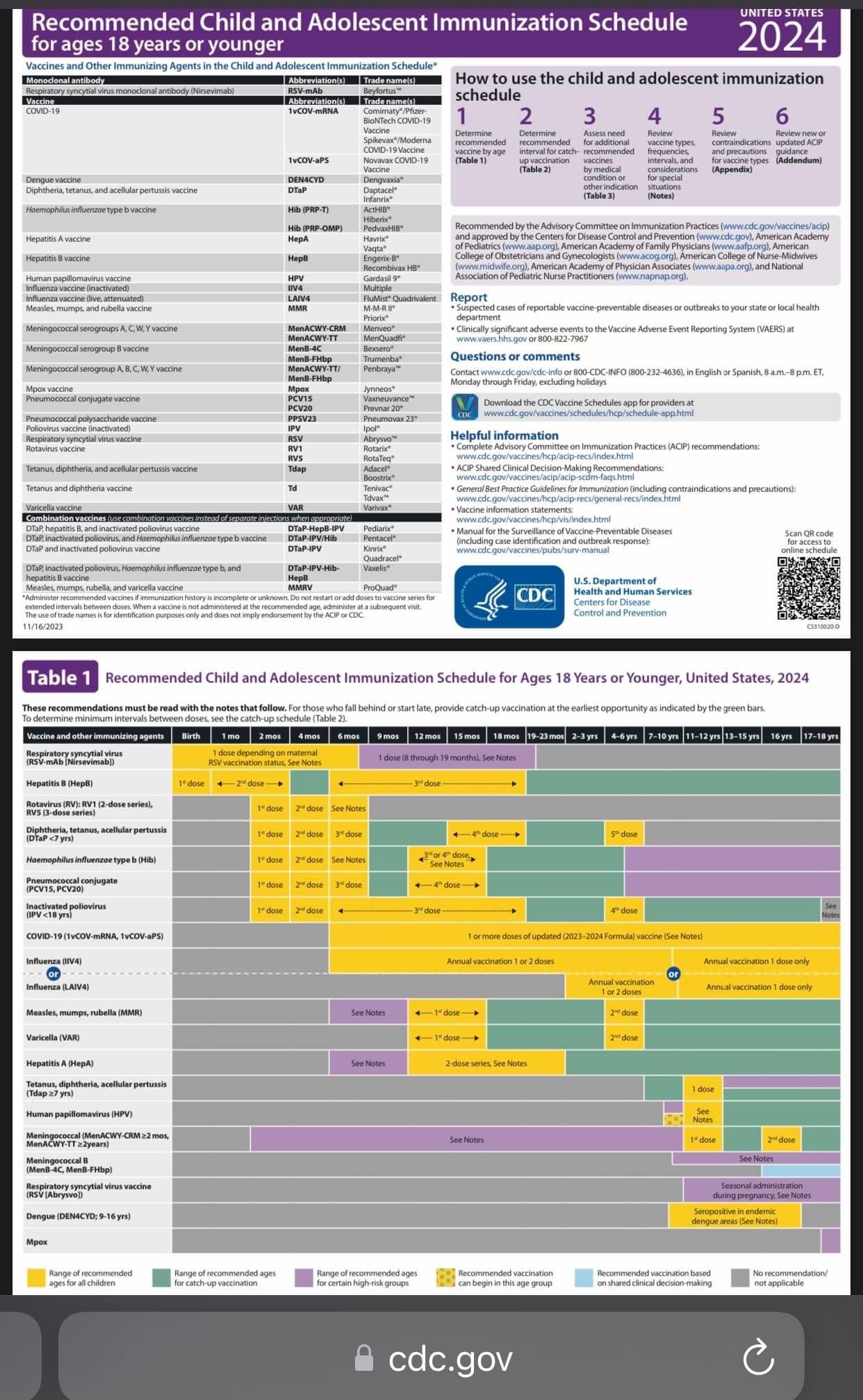
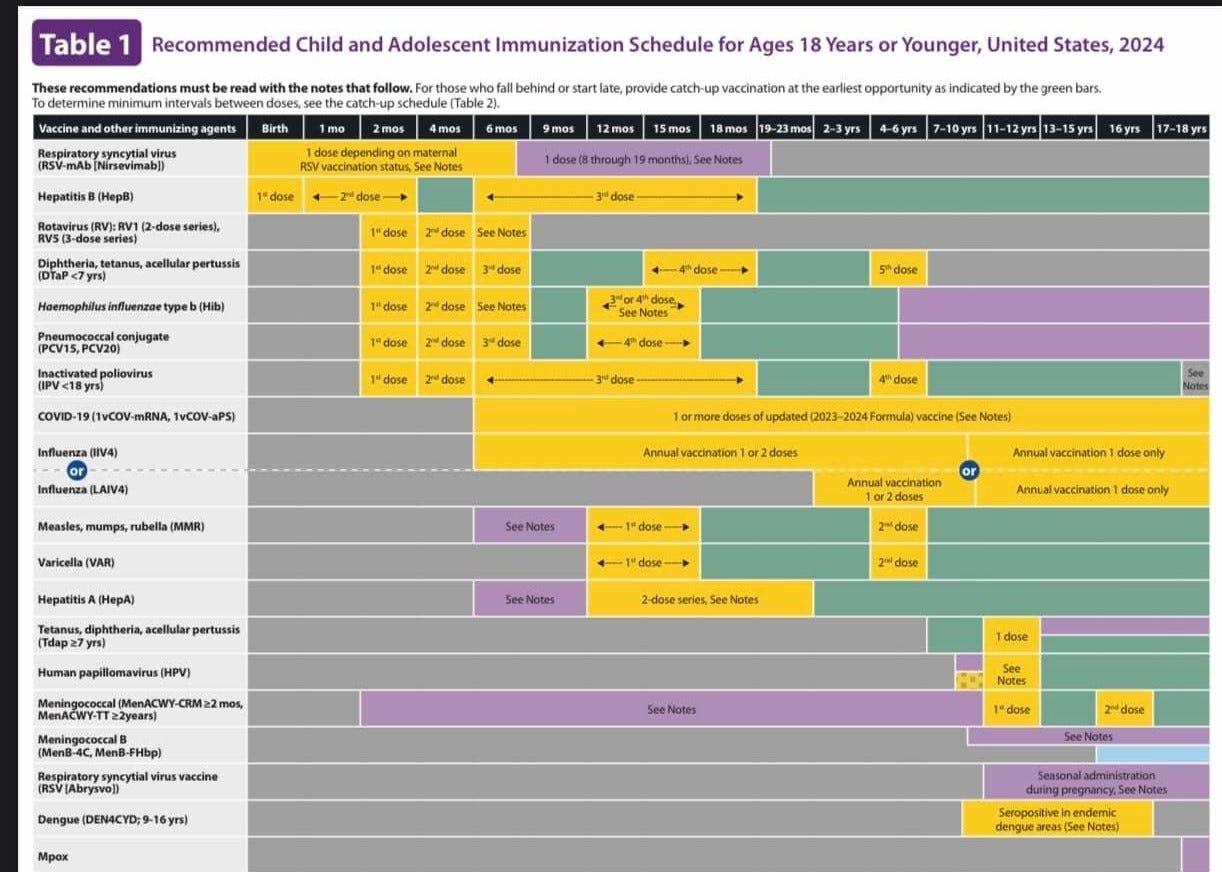
Here is the CDC’s Childhood Vaccination Schedule for 2024:
Have you ever heard of ASIA? No, not the continent. This ASIA is Autoimmune/Inflammatory Syndrome Induced by Adjuvants. The syndrome was first described in a study published in 2011. The authors include Dr. Yehuda Schoenfeld - the guy who literally wrote the book - the medical textbook - on Vaccines and Autoimmunity. An updated review of ASIA was published in this 2023 article from the peer-reviewed medical literature.
From the 2023 article:
Through the ASIA syndrome International Registry (established in 2011) up to December 2016, 300 patients were identified [26]. The mean age at disease onset was 37 years, and the mean duration between adjuvant stimuli and the development of autoimmune conditions was 16.8 months (a range of: 3 days to 5 years). Arthralgia, myalgia, chronic fatigue, sleep disturbances, weakness, sicca symptoms, fever. Arthritis and neurological manifestations were the most frequently reported symptoms. Clinically well-defined diseases were observed in 89% of patients. Undifferentiated connective tissue disease (UCTD) was the most frequent disease, followed by fibromyalgia and/or chronic fatigue syndrome. Other autoimmune diseases that were observed included: SLE, vasculitis, mainly giant cell arteritis (GCA), ANCA-associated vasculitis, Behçet's disease, Henoch-Schoenlein purpura, polyarteritis nodosa, and cutaneous sarcoidosis. Cases of type 1 diabetes mellitus (DM1) were related to exposure to the HBV (Hepatitis B Vaccine) and HPV vaccines, whereas autoimmune liver diseases were associated with HBV vaccination. In the HBV group, the most frequent diagnosis was UCTD; in HPV, fibromyalgia; and in influenza, UCTD or GCA. The materials identified as adjuvants were: cosmetic fillers of mineral oil, hyaluronic acid, polyalkylimide (PAL), polyacrylamide gel (PAC) and collagen. Metallic implants and silicone breast implants were also found. Vaccines identified as adjuvants were hepatitis B virus (HBV) vaccine, human papillomavirus (HPV) vaccine, influenza vaccine, and other vaccines (hepatitis A virus; diphtheria, tetanus, pertussis, measles, mumps, and rubella [27].
Between 2011 and 2016, 4479 ASIA cases have been identified [28]. Severe cases of ASIA were mostly associated with HPV vaccine, influenza vaccine, silicone, and mineral oil injections [28].
Well. That’s interesting. In the published studies on ASIA, the aluminum adjuvants used in vaccines are most often cited as being responsible for the inflammatory response that leads to the autoimmune reaction. The HPV vaccine that was originally studied was the quadrivalent, original version of Gardasil, which contained 225 micrograms (mcg) of aluminum. Gardasil 9 contains more than twice the amount of aluminum, with “approximately 500 mcg.” The adult formulation of the hepatitis B vaccine contains 500 mcg. of aluminum. As noted in the write-ups for ASIA, vaccines for diphtheria, tetanus, and pertussis (DTaP and Tdap) were also implicated in the onset of the autoimmune/inflammatory syndrome, and these vaccines also contain aluminum, in amounts ranging from 500 mcg. (Infanrix and Kinrix) to 850 mcg. per dose (Pediarix).
What’s interesting to me is that in the descriptions of ASIA (the syndrome), the patients who have received diagnosis and who have participated in the studies are adults, with the exception of some in the older adolescent range, who were diagnosed with ASIA after HPV vaccines.
What about babies and young children? If 500 mcg of aluminum in a Gardasil vaccine or a Hepatitis B vaccine can cause the onset of Autoimmune/Inflammatory Syndrome Induced by Adjuvants in an ADULT, what is aluminum in vaccines doing to tiny infants and young children?
Let’s go back for a minute and look again at the CDC’s Childhood Vaccination Schedule. What happens at those “well-baby” checks?
At birth: Hepatitis B vaccine: 250 mcg aluminum
2 months: Hep B (250 mcg), DTaP (330 - 625 mcg, depending on the manufacturer), HiB (225 mcg), pneumococcal (125 mcg). If the combo shot for DTaP, inactivated polio, and Hep B is used, that’s 850 mcg. aluminum.
Total at 2 months: 930 - 1,200 mcg. aluminum
4 months: DTaP, HiB, pneumococcal (680 - 975 mcg.) Note: Many children also receive the Hepatitis B vaccine at the 4-month appointment because they are being given the combo shots. If this is done, the total aluminum is the same as at the 2 month appointment: 930 - 1,200 mcg.
6 months: Same as 2 month appointment. Total: 930 - 1,200 mcg. aluminum.
So, during the first six months of life, infants, who weigh generally weigh between 7 pounds and 17 pounds, are injected with between 2,790 and 3,850 mcg. of aluminum. Is it unreasonable to assume that if 500 micrograms of aluminum can induce a hyperinflammatory response leading to autoimmunity in a 150-pound adult, 2,790 to 3,850 mcg. of aluminum injected into a 7-17 pound baby would also negatively affect the immune system of that infant?
Does the injection of so much aluminum skew the immune system toward a hyper-inflammatory state, so that by the time they receive the MMR vaccine (at 12-15 months of age), they are more vulnerable to serious adverse reactions?
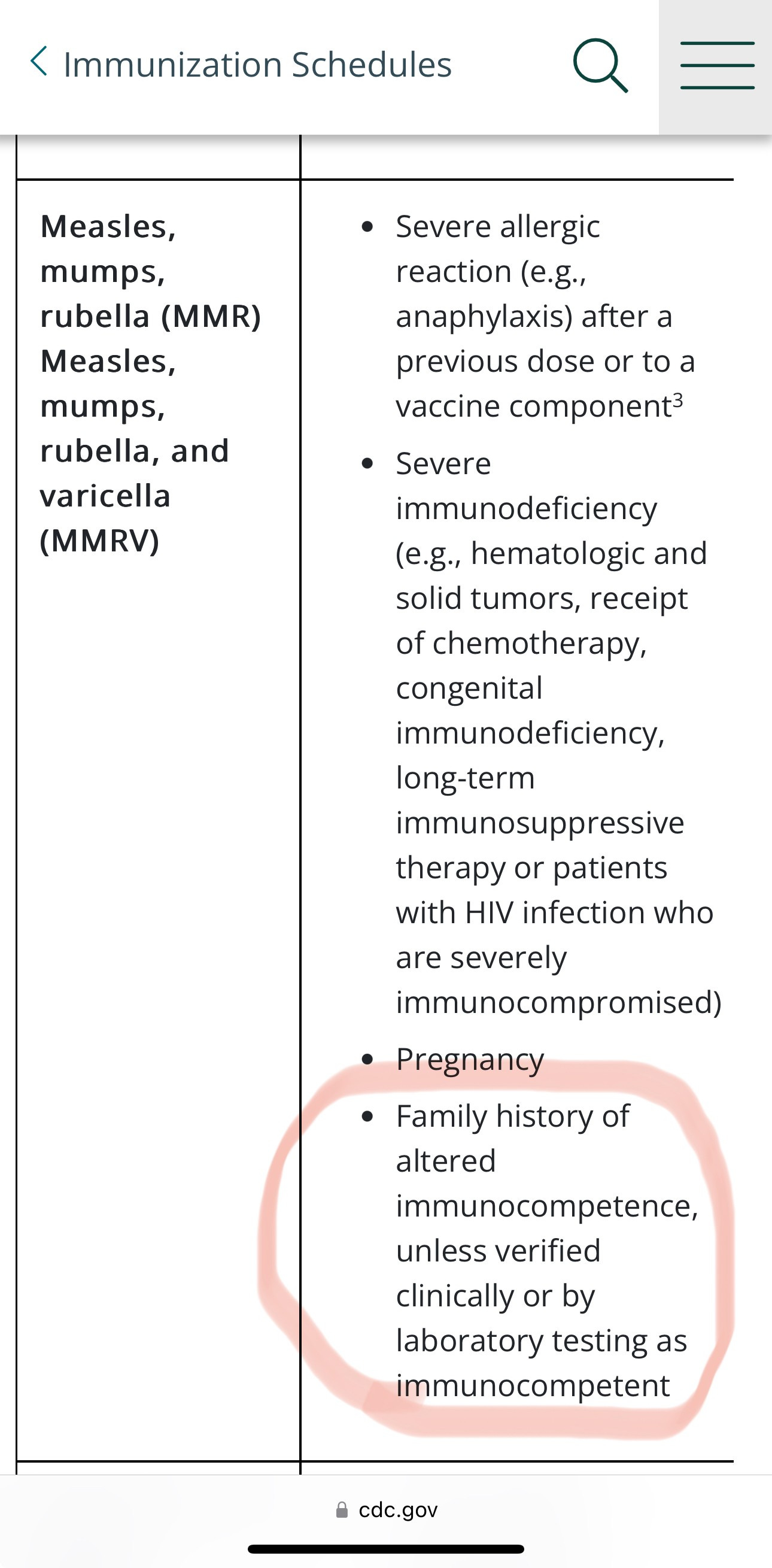
What does the CDC say about who should not receive the MMR?
MMR contraindications from CDC: Child Immunization Schedule Appendix| CDC
Are children whose parents have aberrations in their immune system function more vulnerable to serious vaccine injury, and therefore, more likely to be diagnosed with an autism spectrum disorder? The research certainly supports this as being highly likely. And yet, the mainstream media and allopathic medical experts strongly urge family members (including babies and children) to receive vaccinations “in order to protect those who cannot be vaccinated.” What about the fact that those children are at increased risk of serious adverse reactions, due to their OWN predisposition to immune dysfunction?
And what about those children who do not have strong family histories of immune dysregulation, including autoimmune disease? Are they also at increased risk of immune system problems? Why is the birth to five-year age group showing the highest number of primary immune disorders?? What is happening to these children to skew their immune systems???
What happens to children between birth and age five, that could affect their immune systems? Vaccines. They alter the immune system. It’s what they are DESIGNED to do. When vaccine trials are conducted on healthy children and when they exclude children who do not have “normal” immune systems, there is literally zero data on how those vaccines will affect children whose genetics put them at increased risk of immune deficiency or autoimmune disorders. When a child has a genetic predisposition to autoimmunity (family history), it should come as no surprise when that child reacts differently to vaccines that were studied on children who did not have that same genetic predisposition.
Please watch the following video…
We know that the CDC and Merck (maker of the MMR II vaccine) advise against vaccinating immune compromised individuals because these individuals have a higher risk of serious adverse reactions to the MMR vaccine. They even say that FAMILY MEMBERS of people with immune system disorders SHOULD NOT BE VACCINATED UNTIL IMMUNE COMPETENCE IS VERIFIED BY LABORATORY ANALYSIS.
I would love to ask my friends, especially those friends who have autoimmune diagnoses and/or primary immune deficiency diagnoses, if they were EVER told that the MMR vaccine should NOT be given to their babies and children. Maybe it’s happened? I’ve never heard of it happening, and I believe the reason is because the vast majority of doctors and nurses have never read a vaccine manufacturer’s insert. They are told: (1) Vaccines are the greatest miracle in the history of mankind; (2) Give them exactly according to the schedule; (3) Give as many as you can at one time, because that way, you don’t have to worry if the parents will come back; (4) Anyone who questions the safety or efficacy of vaccines should be ridiculed, belittled, and shamed, and if that doesn’t work, threaten to call CPS for medical neglect. (Yes. That has happened. The best way to avoid it is to stay away from pediatricians.)
So, what happens when immune compromised babies and young children receive the MMR vaccine?
Here are a couple of examples from the published medical literature.
1. 21-month-old boy. Vaccine strain measles virus found in the brain. 51 days in hospital at which point he died.
We report a case of measles inclusion-body encephalitis (MIBE) occurring in an apparently healthy 21-month-old boy 8.5 months after measles-mumps-rubella vaccination. He had no prior evidence of immune deficiency and no history of measles exposure or clinical disease. During hospitalization, a primary immunodeficiency characterized by a profoundly depressed CD8 cell count and dysgammaglobulinemia was demonstrated. A brain biopsy revealed histopathologic features consistent with MIBE, and measles antigens were detected by immunohistochemical staining. Electron microscopy revealed inclusions characteristic of paramyxovirus nucleocapsids within neurons, oligodendroglia, and astrocytes.
The presence of measles virus in the brain tissue was confirmed by reverse transcription polymerase chain reaction.
The nucleotide sequence in the nucleoprotein and fusion gene regions was identical to that of the Moraten and Schwarz vaccine strains; the fusion gene differed from known genotype A wild-type viruses. (source)
“He had NO PRIOR EVIDENCE OF IMMUNE DEFICIENCY.”
2. This article reports the case of a little boy who started developing symptoms of an autoimmune attack on his brain four months after receiving the MMR vaccine at 14 months of age. Four months after receipt of the MMR, he was diagnosed with SCID (Severe Combined Immune Deficiency Syndrome). He was diagnosed with autoimmune haemolysis and developed a persistent H1N1 infection. He received successful Stem Cell Therapy and his immune system improved, but six months after Stem Cell Therapy he started regressing and losing cognitive abilities, motor skills, and language. He developed seizures. His hearing was affected and he developed personality changes and behavioral changes.
After multiple hospitalizations, he died at 69 months of age.
From the report:
Using deep sequencing of fresh brain biopsy material, we identified the Jeryl Lynn 5 mumps virus (MuVJL5), a component of the measles, mumps, rubella (MMR) vaccine that had been administered to the child before the diagnosis of SCID. Similar to findings in measles viruses recovered from cases of SSPE, the mumps virus genome from the brain showed evidence of biased hypermutation, particularly in the matrix (M) gene. Comparison with sequence data from the original vaccine batch used to immunise this child identified the expansion of variants present at low frequency in the vaccine as well as de novo fixed missense substitutions. This case represents the first conclusive demonstration of chronic panencephalitis due to [vaccine strain] mumps virus.
Chronic panencephalitis due to the MMR vaccine. And yes... it was the same strain used in vaccines in both the UK and the US. To be clear: the little boy was vaccinated at 14 months with MMR. He did not have a diagnosis of immune system deficiency until four months AFTER being injected with the MMR vaccine. He suffered for FOUR YEARS AND SEVEN MONTHS before he finally died from chronic panencephalitis, which was CAUSED by the MMR vaccine.
What about Atypical Measles?
“You can’t get the measles from the MMR vaccine.”
“You can’t get Autism from the MMR vaccine.”
Both of these statements are untrue. Atypical measles is listed in the MMR vaccine insert as an adverse reaction from the vaccine.
We don’t know how often this happens because once doctors know the child has been vaccinated, it’s not counted as measles. Even though IT’S MEASLES
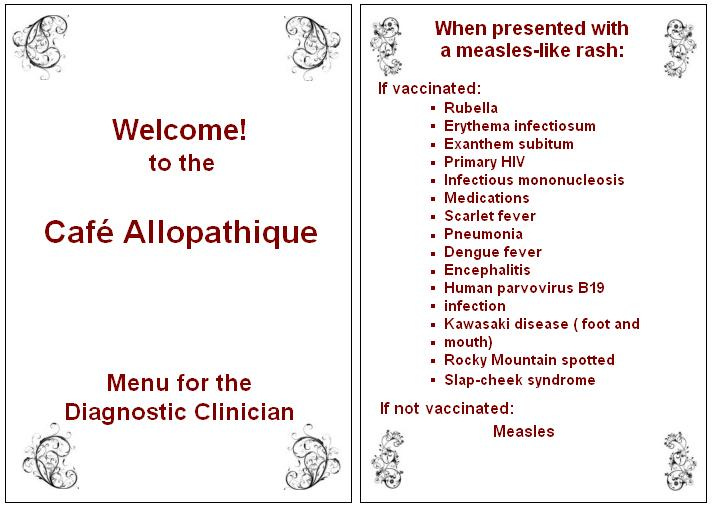
(Credit and thanks to Shawn Siegel for the above graphic)
The MMR vaccine is a Live-Virus vaccine. It can and does cause the measles. Those who have atypical measles from the vaccine may not always have the rash, but they can still be contagious to others, just as those who are vaccinated against pertussis can be infected and spread the infection to others, even in the absence of symptoms.
Here are a few citations from the published medical literature...
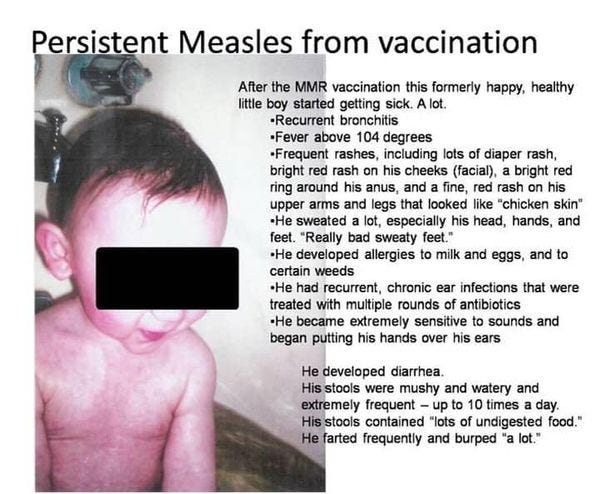
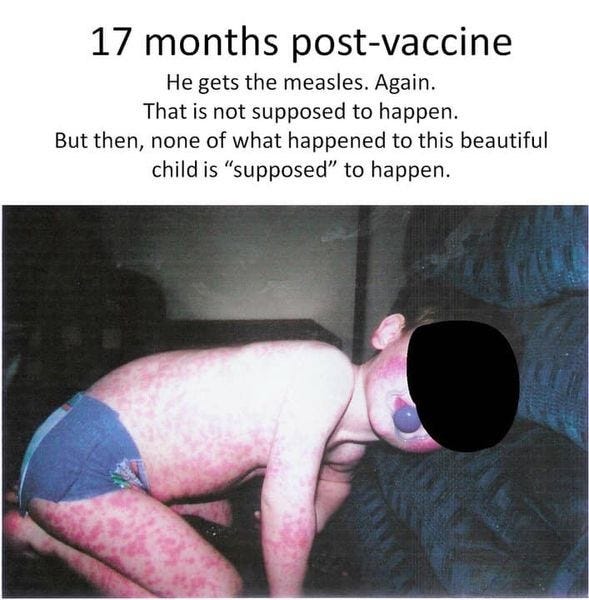
Atypical Measles from MMR Vaccination:
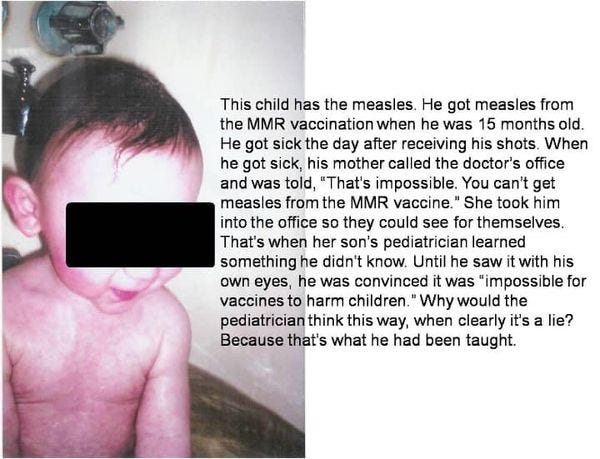
The child in these photos not only got the measles from the MMR vaccine. He was also diagnosed with autism, after his health and development tanked, following the MMR vaccine.
Neither case of measles was ever reported to the state health department. I know that because I saw this child in private practice in Indiana. I reviewed his medical records and the timeline. There were zero cases of measles reported in Indiana during the years this happened.
Why wasn’t this reported? Because it didn’t suit the narrative that “vaccines are safe and effective.”
Bottom Line: Who should NOT get the MMR vaccine?
Anyone with personal or family history of compromised immune system.
Anyone who is showing signs of a compromised immune system, as evidenced by recurrent infections.
Anyone who has done their research and who understands that measles can be good for you and has beneficial effects on the immune system that can help fight cancer and autoimmune disease later in life.
Anyone who understand that complications from measles are due to nutritional deficiencies (especially deficiencies of vitamins A and C).
Anyone who has a strong conviction against abortion and the pharmaceutical industry’s profiteering from the remains of aborted fetuses. And anyone who is concerned about insertional mutagenesis and what that does to children injected with the DNA fragments of other human beings. Go here for more on this.
More on measles and the MMR vaccine:
Thank you Marcella.
Yesterday, I just happened to listen to the mainstream news whilst driving. They reported that 10% of children getting measles will have severe outcomes…..ie. go get the shots. I was stunned. Naturally many people will believe this and feel that they are doing the best thing for their precious children. Very sad.
Great round up on immune deficiency, needs to be shared with everyone, especially those starting a family.