


Let's Talk About Tetanus
Do you need a booster? Is the Tdap in pregnancy safe?

Note: This article is about tetanus. There is no such thing as a “tetanus shot” anymore. The manufacturers stopped making the single tetanus shot in 2012. Since that time, getting a “tetanus shot” means getting either a DTaP or Tdap, depending on the person’s age, with DTaP being the option for infants and children up to age 7 years. Tdap is the version that is given to adults and children aged 7 and up. Tdap is also the one given to pregnant women. Because we cannot talk about the “tetanus shot” without discussing DTaP and Tdap, this article presents information about the childhood and adult vaccines, focusing more on the Tdap, particularly with regard to “tetanus boosters” and Tdap given to pregnant women.

“Help! My child cut herself on a piece of broken glass while washing dishes and she needs stitches. We are in the Emergency Room. They want to give her a tetanus shot. I’m scared. We don’t vaccinate, but the thought of tetanus is terrifying! What should I do???”
“Help! My husband was building a fence in the backyard of our suburban home, and he stepped on one of the nails. It went through his tennis shoe and left a puncture wound in his foot. It bled a lot, but we are concerned about infection, so we went to the doctor just to be sure he doesn’t need an antibiotic. They want to give him a tetanus shot. It was a new nail, purchased last week from Home Depot. Does he need a tetanus shot??”
And my personal favorite…
“My thirteen-year-old got stung by a bee. The pediatrician wants to give him a tetanus shot. Do bee stings cause tetanus???”
For the record…

(source)
Why in the world would a “tetanus shot” be given after a bee sting, you may ask? Because it is recommended. Apparently, that recommendation comes from an article published in 1879, which reported on a case of tetanus in a 34-year-old man who developed tetanus and who also had been stung by a bee “a couple of weeks prior.”
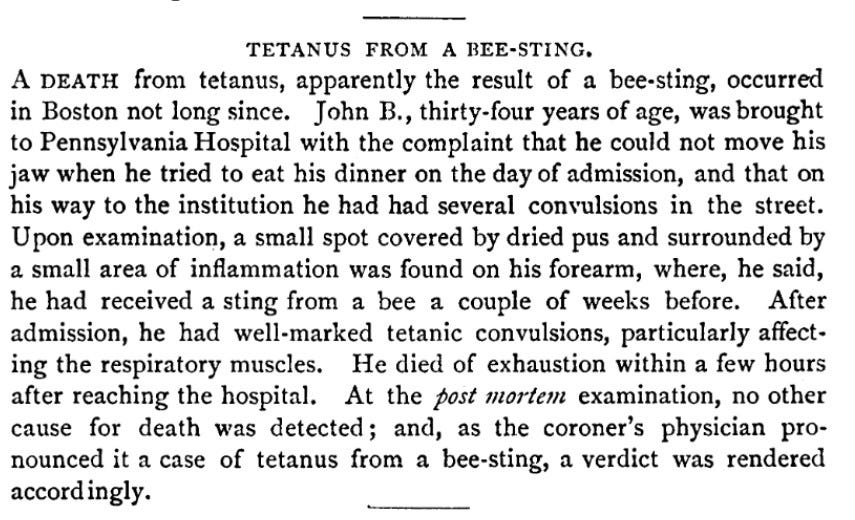
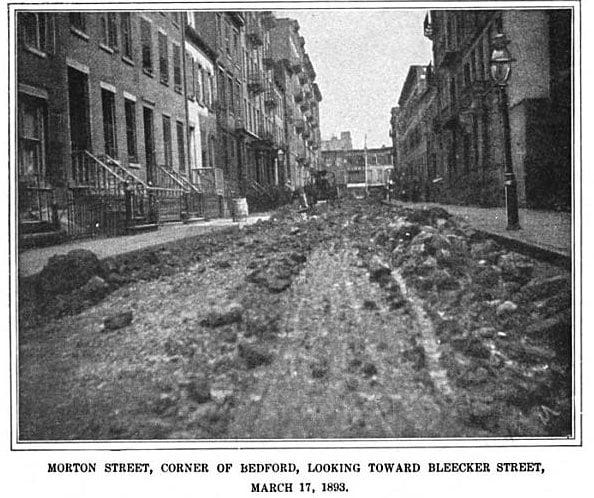
Well. That IS terrifying. Of course, we don’t know what John B. did during those weeks after the bee sting and prior to the onset of tetanus. Given that it was 1879 - prior to the invention of cars, and during a time when manure from horses was literally everywhere… and given the high probability that he did not have any antibiotic ointment or a band-aid to cover the sting, one might surmise that it was not the sting itself that caused the tetanus. It is likely that at some point following the sting, John B. was in the presence of horse manure, which he would have likely come into contact in if he walked anywhere or if he, himself owned a horse. If he set foot in the streets of any Northeastern city, he would have certainly gotten horse manure on his boots, and very likely on his clothing from the mixture of mud and manure that was everywhere in the streets of Boston, New York, and other major cities in the Northeastern United States at the time.
The scenarios quoted at the beginning of this article are illustrative of some of the many messages I have received through Facebook Messenger over the last fourteen years, since I started writing on FB about vaccines. Many people who do not vaccinate themselves or their children are terrified of tetanus. I have lost track of the number of times I have heard, “Tetanus is the ONE thing I’m really concerned about.” This statement often comes from friends who live on farms, who have horses and cows, or whose children participate in horseback riding as an activity. Because tetanus bacteria lives in the fecal matter of horses, cows, and other large mammals, the increased concern about tetanus in these environments is justified. However, if you live on a farm and you are concerned about tetanus, don’t go running to the doctor’s office asking for the vaccine just yet… Read on…
The many questions I have received about tetanus have spurred a few Facebook posts like this one:

Tetanus used to be a significant concern in the United States, back in the day before automobiles were invented and the streets were a stinky, sticky mixture of horse shit and mud. There are some really good write-ups on the history of tetanus and the vaccine. This one from Circle of Mamas is excellent. So is this one from National Vaccine Information Center. I encourage you to read both of these articles. After you finish here, please.
Did vaccines save us from tetanus?
As is the case with all “vaccine preventable” infections, those who benefit from the sale and uptake of vaccines try to take credit for the reduction in cases and deaths from tetanus. As this graph, from the Circle of Mamas article linked above shows, vaccines did not save us from tetanus.

The graph above is not an isolated scenario. As the two graphs below show, the decline in deaths from infectious diseases had little to do with vaccination, and a lot to do with improvements in sanitation (no more manure in the street, improvements in plumbing and clean water), and improvements in living conditions and nutrition. A really good resource for learning about this is the book, “Dissolving Illusions” by Dr. Suzanne Humphries and Roman Bystrianyk. If you want to take a quick look at the living conditions in American cities during the latter part of the 1800s, this is a great website. One quick perusal and you will easily see why infectious diseases were rampant in places like New York City and Boston prior to 1900s.
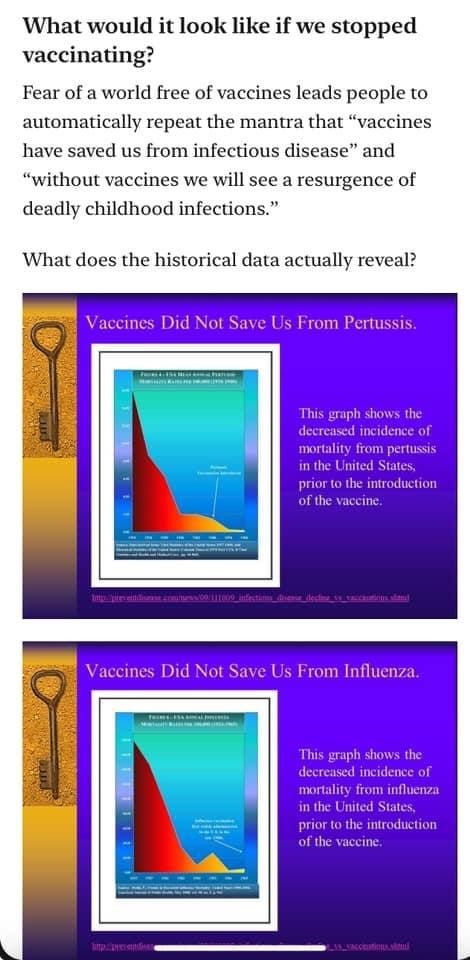
Note: Pertussis (whooping cough) and influenza are just two examples of infectious diseases for which the death rate had dropped more than 98% prior to the release of the vaccine that is said to have resulted in the reduction of deaths from said infection. If you want to learn more, please check this post - when you finish here, please.
When considering whether or not you should get a vaccine, you really should do a cost-benefit analysis that includes looking at the risk of serious outcomes, including death from the infection vs. the risks of serious outcomes, including death, from taking the vaccine.
What are your chances of dying from tetanus if you currently live in the United States?
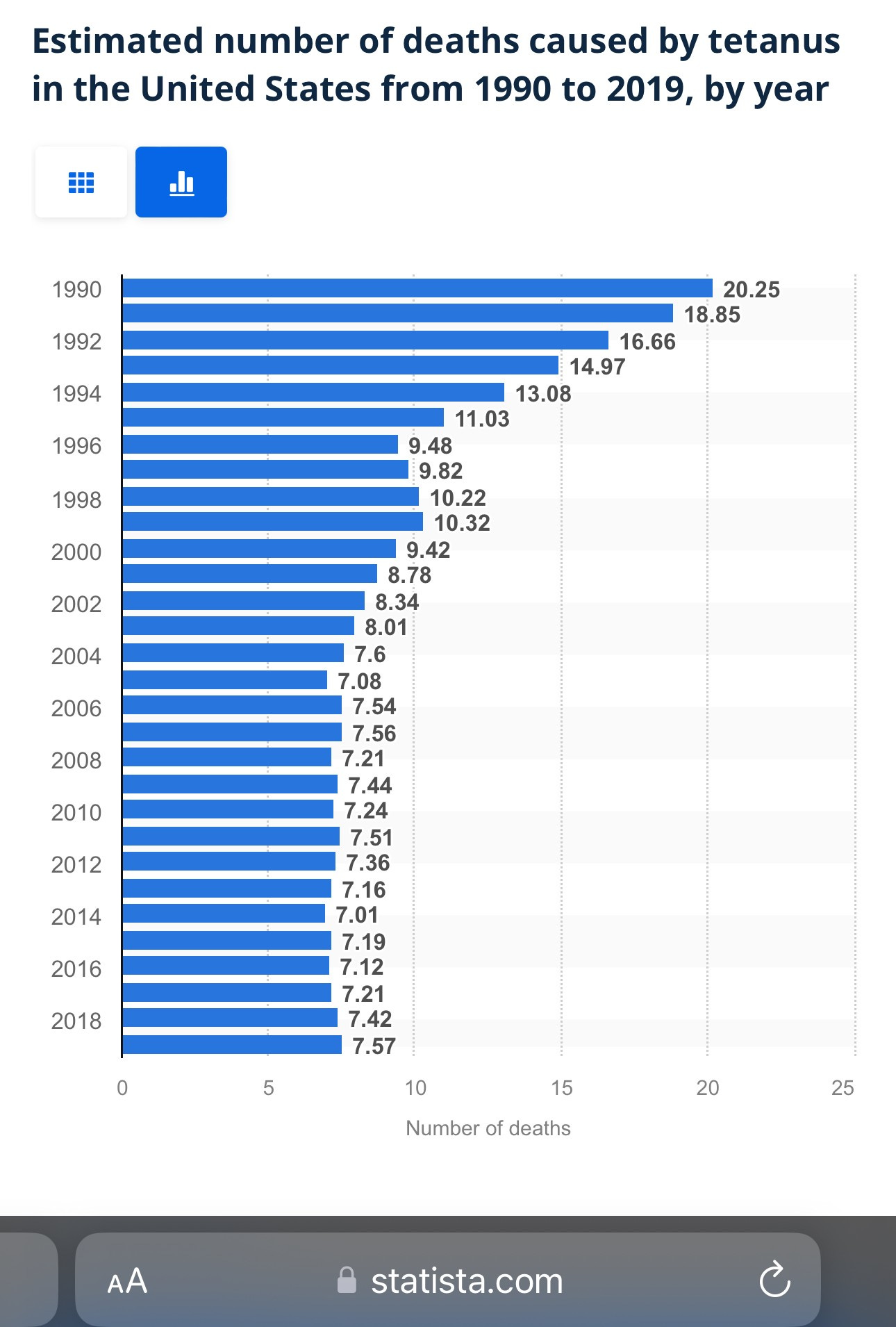
“Since 1999, the number of deaths caused by tetanus in the United States has not exceeded 10 in a given year. This statistic shows the number of deaths caused by tetanus in the U.S. from 1990 to 2019.” (source)
As the above graph shows, the yearly average number of deaths from tetanus in the U.S. over the last twenty years is 7.5. In order to calculate your risk of death from tetanus, we need to know how many people live in the United States. According to the 2020 census data, that number is 329.5 million.

Dividing 329,500,000 (the number of people living in the U.S.) by 7.5 (the yearly average of deaths from tetanus) yields the following:
Your odds of dying from tetanus if you live in the United States are 1 in 43,933,333.333. Roughly, 1 in 44 million. Have you ever heard the ridiculous statement that serious vaccine injuries are 1 in a million? IF that were true (it’s not… ), that would mean your odds of serious injury from “tetanus” vaccination would be 44 times higher than your odds of dying from tetanus.
Tetanus is still a scary thing for some people. Part of the reason is because we have been told there is no cure for tetanus. Here is what the Mayo Clinic has to say:
Tetanus is a serious disease of the nervous system caused by a toxin-producing bacterium. The disease causes muscle contractions, particularly of your jaw and neck muscles. Tetanus is commonly known as lockjaw.
Severe complications of tetanus can be life-threatening. There's no cure for tetanus. Treatment focuses on managing symptoms and complications until the effects of the tetanus toxin resolve.
Because of the widespread use of vaccines, cases of tetanus are rare in the United States and other parts of the developed world. The disease remains a threat to people who aren't up to date on their vaccinations. It's more common in developing countries. (source)
Is it true there is no cure for tetanus? No.
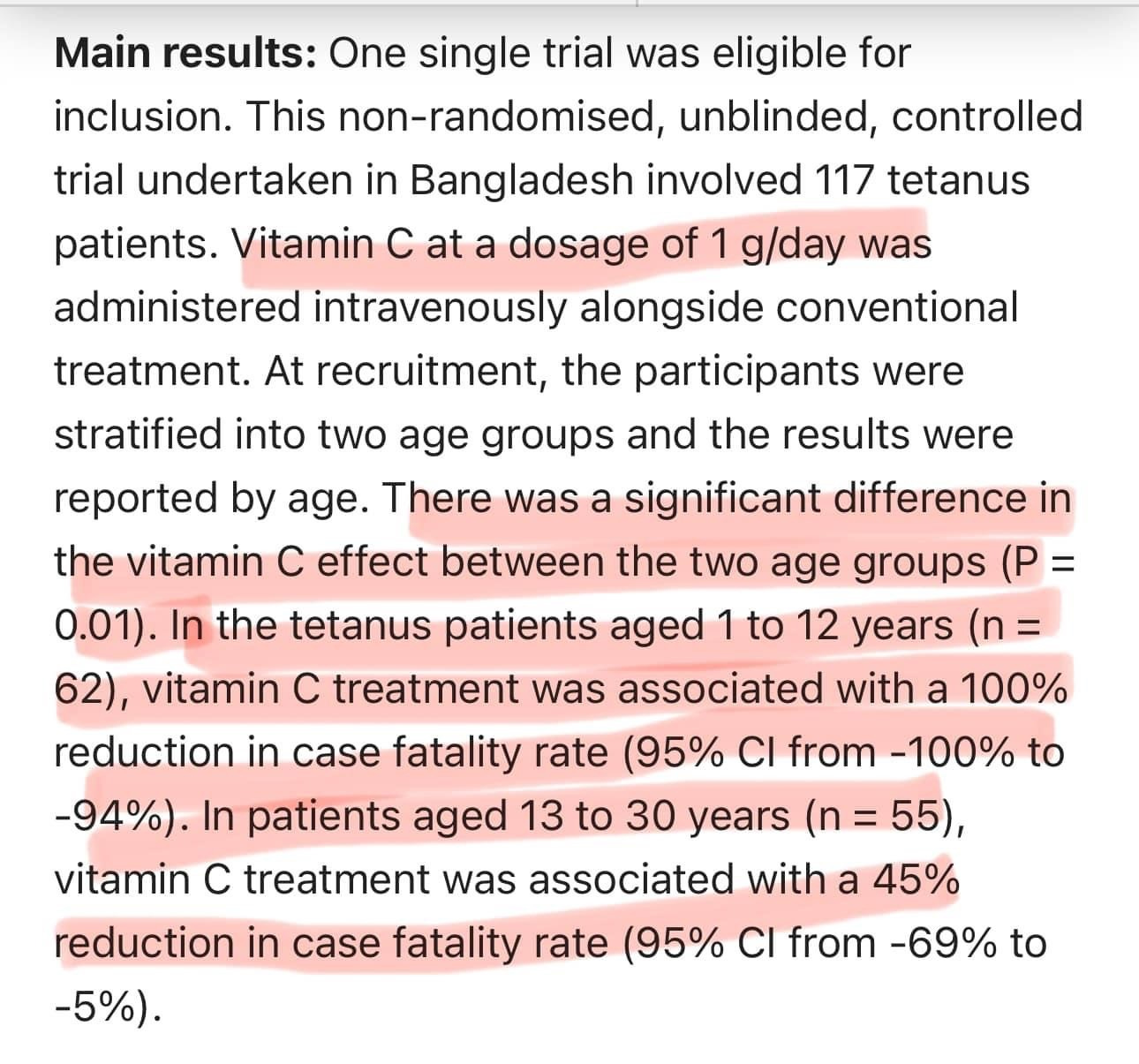
In this study, IV vitamin C (one gram per day) resulted in a 100% reduction in case-fatality rate in patients 12 years and under, and a 45% reduction in case-fatality rate in patients aged 13-30 years. The lower efficacy in older teens and adults is most likely because the dose was not high enough.
But my doctor says I need a booster every 10 years. Is this true? NO.
Given that the World Health Organization (WHO) does not recommend tetanus boosters AT ALL for adults who have received the initial childhood series, why does the CDC continue to recommend boosters every ten years?
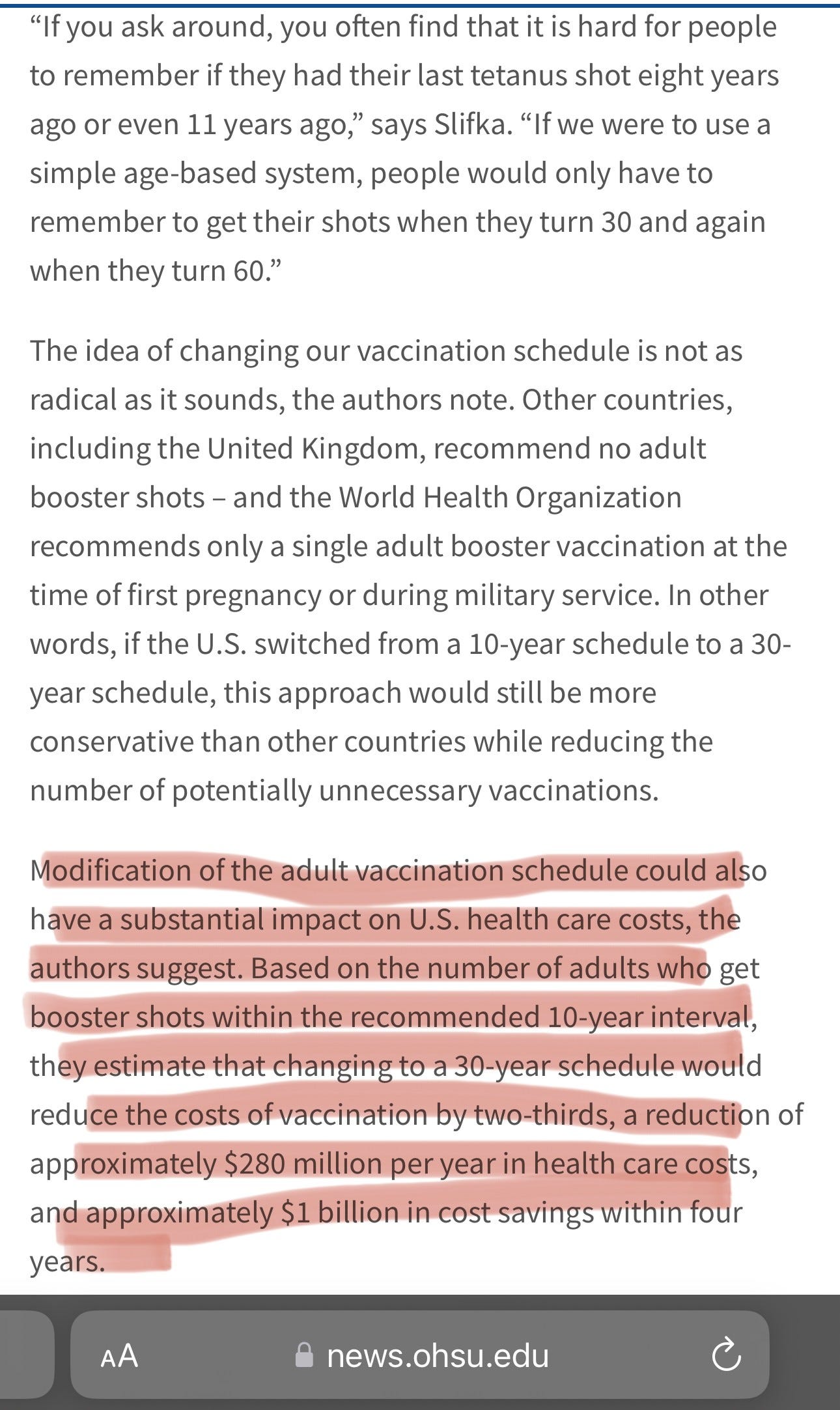
That’s right. The authors of the study suggest changing the adult schedule to recommend boosters every 30 years instead of every 10 years, as is currently recommended. They note that doing so would save an estimated $280 million per year and over $1 Billion in health costs over four years.
That recommendation was made in 2016. Eight years ago. Nothing has changed. And the reason is because the pharmaceutical industry and their minions in the government agencies that make the recommendations don't care about the health (physical or financial) of America or our citizens. The $2 Billion that could have been saved went into their pockets.
What we know so far…
If you live in the United States (or other developed nations) your risk of dying from tetanus is roughly 1 in 44 million.
Vaccines had little to do with the reduction of death from tetanus. Improvements in sanitation, the invention of the automobile, and the resulting the shift away from horse poop in the streets had a lot more to do with the reduction in cases and deaths from tetanus.
The pharmaceutical lobby and the U.S. government agencies who benefit financially from the sales of vaccines and who also make the recommendations for their use, via the child and adult schedules have chosen to ignore the recommendations of the World Health Organization (WHO) and scientific studies that show there is ZERO need for tetanus boosters every ten years, and in continuing to recommend boosters every ten years, they have increased their sales by an estimated $2 Billion over the last 8 years. For something that is completely unnecessary, and which is not without significant risk.
What ingredients of concern are found in tetanus-containing vaccines?
Here is where you can find the vaccine manufacturer’s inserts for all licensed vaccines in the United States. And below are links to the DTaP and Tdap vaccines, which is what you will receive if you consent to a “tetanus shot:”
DTaP Vaccines:
Infanrix: 500 micrograms (mcg.) aluminum hydroxide, </= 100 mcg. formaldehyde, </= 100 mcg. Polysorbate 80 (TWEEN).
DAPTACEL: 1.5 mg aluminum phosphate (333 mcg. of aluminum), ≤5 mcg formaldehyde, <50 ng residual glutaraldehyde and 3.3 mg (0.6% v/v) 2-phenoxyethanol.
Tdap Vaccines:
Adacel: 1.5 mg aluminum phosphate (333 mcg. of aluminum), ≤5 mcg formaldehyde, <50 ng residual glutaraldehyde and 3.3 mg (0.6% v/v) 2-phenoxyethanol.
Boostrix: 300 micrograms (mcg.) aluminum hydroxide, </= 100 mcg. formaldehyde, </= 100 mcg. Polysorbate 80 (TWEEN).
Occasionally, I will hear someone recommend getting the TD booster, which is Tetanus and Diphtheria, without the pertussis component. The TD vaccine information is listed below:
TDVAX: aluminum adjuvant (not more than 0.53 mg [530 mcg.] aluminum by assay), < 100 mcg of formaldehyde, trace amount of thimerosal [46.9% mercury, (< 0.3 mcg mercury/dose)]
TENIVAC: 1.5 mg of aluminum phosphate (0.330 mcg of aluminum) and ≤5.0 mcg of formaldehyde
As you can see, ALL of the available options contain high amounts of aluminum, with each 0.5 mL dose boasting between 330 and 530 micrograms. Aluminum is used as an adjuvant to cause an inflammatory response, which increases the immune response. You should also know that all of the DTaP, Tdap, and DT vaccines are cultured on casamino acids - cow’s milk protein, and the final product, which is injected into babies, infants, children, and adults, contains cow’s milk protein.
Deaths from Tetanus Containing Vaccines
I just did a quick search of the Vaccine Adverse Events Reporting System (VAERS) to see how many deaths from Tetanus containing vaccines have been reported.
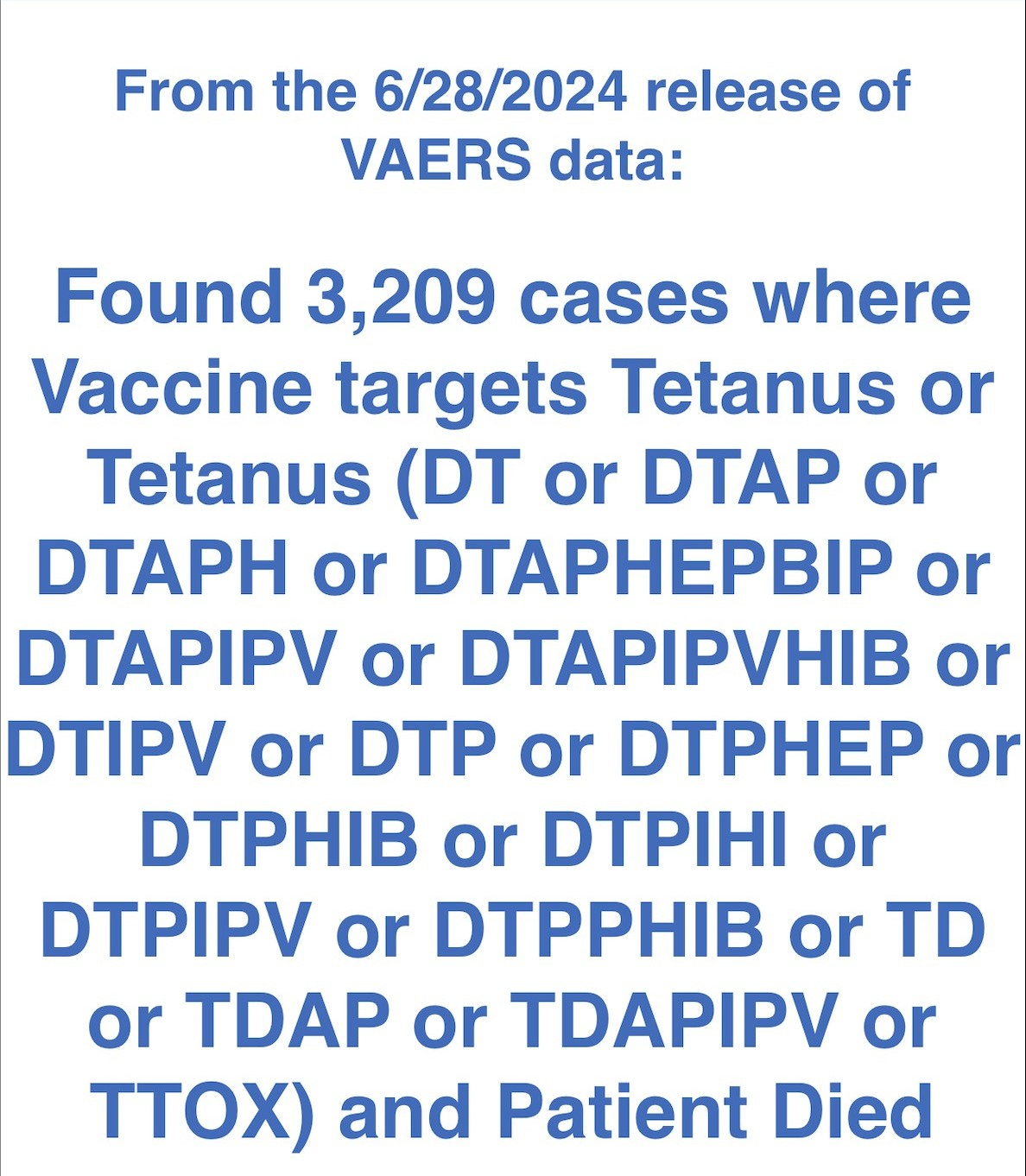
3,209 deaths have been reported to VAERS from Tetanus containing vaccines.
Here is the breakdown by age:

As you consider these numbers, keep in mind that according to a study commissioned by HHS and CDC, conducted between 2007-2010 by Harvard Pilgrim Research Group, less than 1% of even the most serious adverse reactions to vaccines are reported. Let that sink in.
One reason people die from the vaccine is anaphylaxis – a severe allergic reaction to a component of the vaccine. The vaccine-manufacturer’s inserts warn about this, and they state that anyone who has had a previous severe reaction or who has a known allergy to ANY of the vaccine’s ingredients should not receive the vaccine.
How many people do you know with allergies to cow’s milk? There are a lot of them. My daughter is one of them. She nearly died in my arms three hours after a Tdap at age fifteen. I was bullied into giving her a “tetanus shot.” At that time, I didn’t know the information I am giving to you.
This article reports on the observations of a group of physicians who witnessed several cases of anaphylaxis in their patients, following administration of the DTaP vaccine. (Note: The online report states the children received DPT vaccine. This is an error, since the DPT vaccine was no longer in use in the U.S. at the time.) The doctors presented their observations at an annual meeting of the American Academy of Asthma, Allergy, and Immunology in 2011. What I find most interesting is that initially, the doctors (who are trained in allergy and immunology) were shocked to find milk protein in the vaccines they tested. They thought it was due to contamination. They knew that food proteins are not supposed to be injected into the body – they’re supposed to go through the gastrointestinal tract where they can be appropriately broken down. Injecting food proteins into the blood is THE WAY to create serious food allergies and anaphylaxis, and this has been known since the early 1900s and the work of Charles Richet - work for which he received the Nobel Prize in 1913. Well, guess what? It wasn’t contamination. This problem - anaphylaxis from DTaP and Tdap vaccines in people with milk allergies - has been known since at least 2011. Have you heard anything about it? Has your doctor asked if you or your child have a milk allergy before recommending the DTaP or Tdap vaccine? Our doctor knew of my daughter’s milk allergy, but he recommended (pushed) for her to get the Tdap anyway. Why would he do that? He didn’t know. He had never read the manufacturer’s insert, and he didn’t know what he was injecting into my child.
What about Tdap vaccines given to pregnant women? Are they proven to be safe?
The CDC recommends Tdap vaccines during each pregnancy, on the theory that doing so provides “passive” immunity from pertussis to the baby during the first few months of life. However, scientific evidence actually shows that vaccinating the mother during pregnancy has the opposite of the intended effect, with maternal antibodies interfering with the response to vaccines given in infancy and beyond.
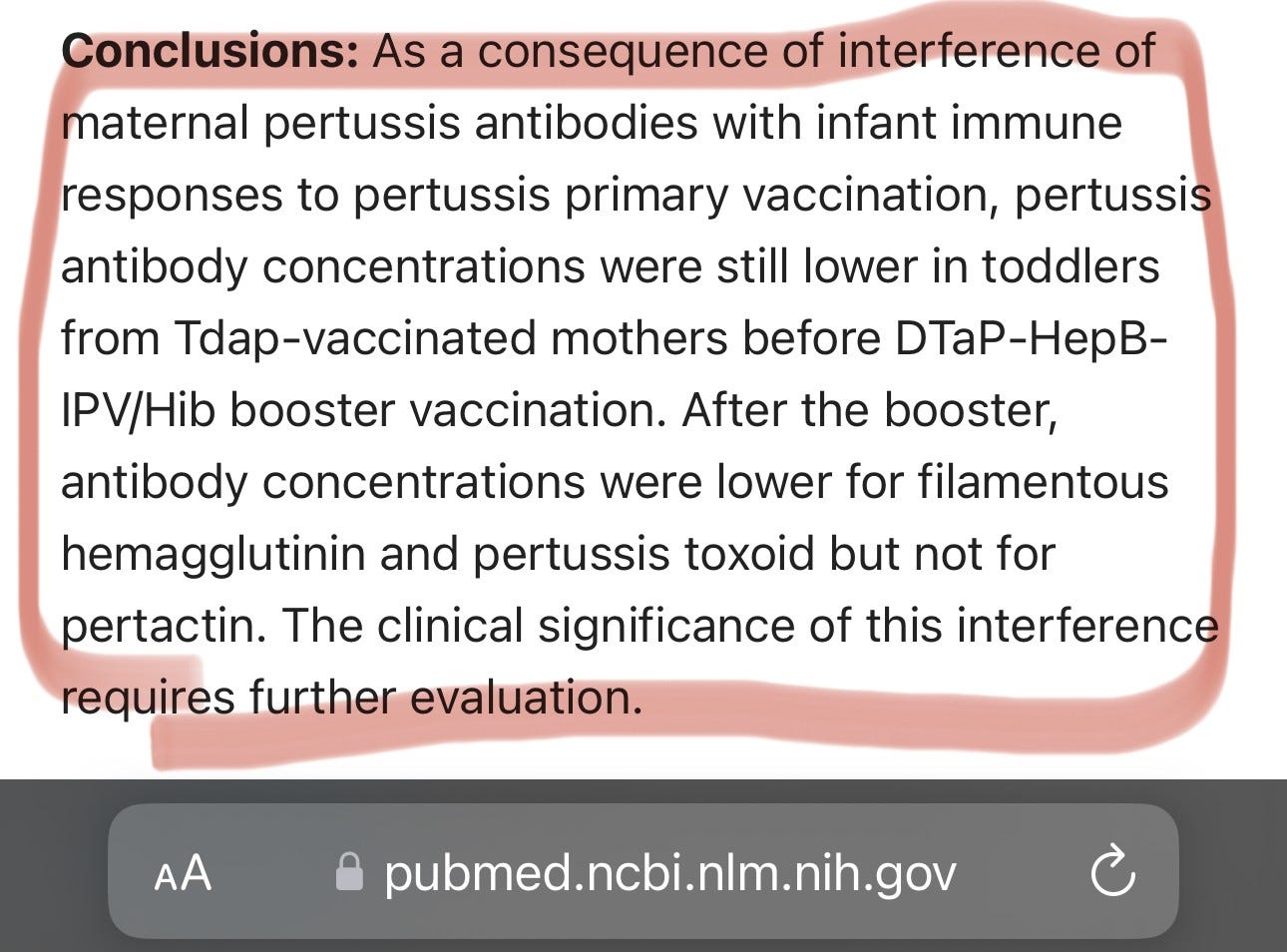
(source)
Has the Tdap vaccine been adequately studied for use in pregnancy? NO.
From the vaccine manufacturer’s insert for Adacel (Tdap vaccine licensed in the United States).

That’s not what your OB/GYN says? That’s because medical doctors (in general) don’t read a lot of research. When they do, they tend to read the abstracts and conclusions. They generally skip over the methods section because medical doctors are not experts in statistics and they (often) don’t understand the methods section. For those who are not familiar with reading published research, the methods section is where you may find things that are very relevant but may be left out of the abstract and conclusions sections (i.e., they are often hidden because their inclusion would not suit the desired outcome or interpretation of the study). Here is an example of the research that has been published for the purpose of showing that Tdap is “safe” in pregnancy…
If you pull up the study on PubMed, this is what you will see:

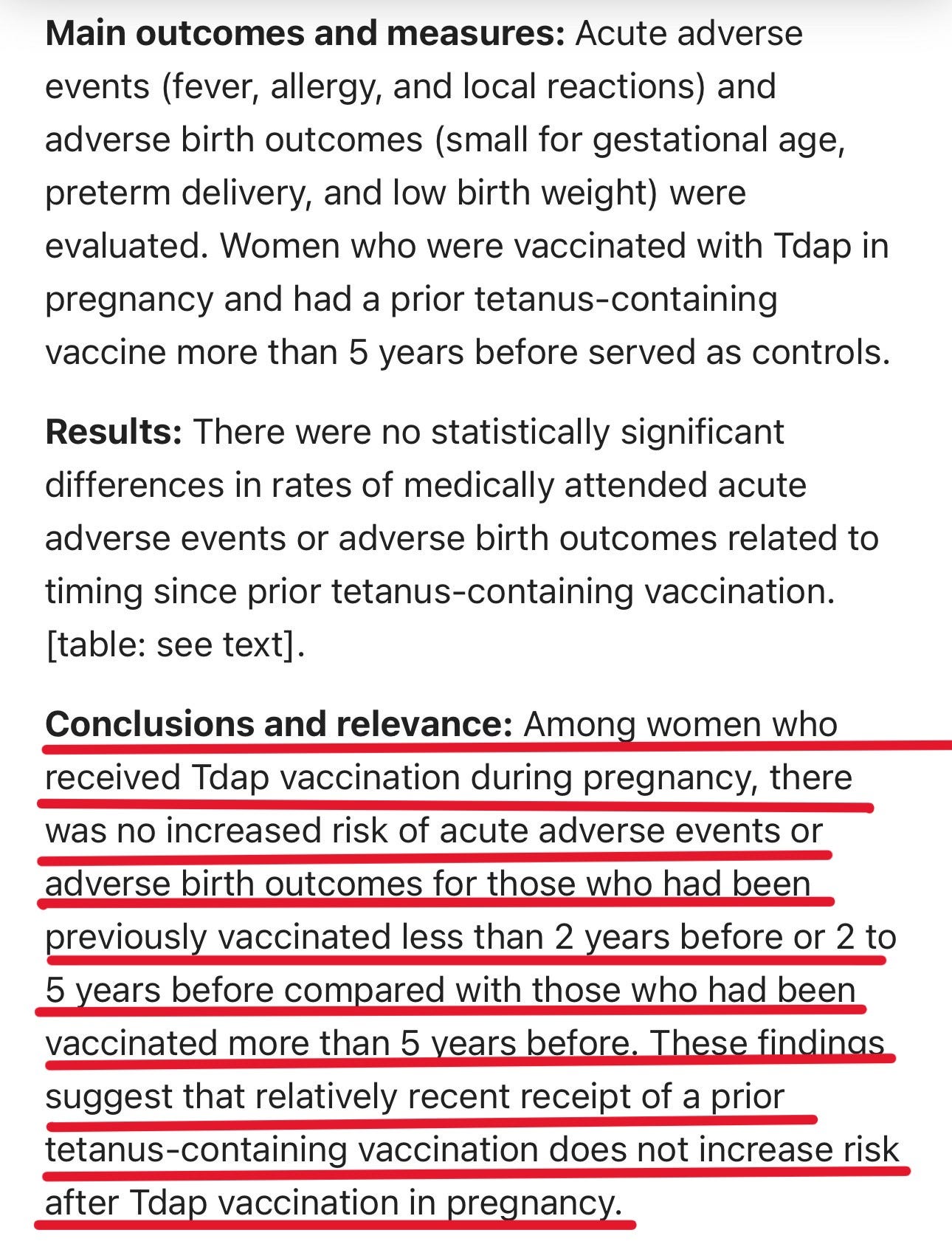
Whew! Reading that, we can be reassured that recurrent Tdap administration in pregnancy is safe, right?
Not so fast…
If you go to the “full text links” and click to read the full study, you can see the methods section. Full texts are often not available without paying for the article. The average price to obtain the article if you cannot access it through your institution/hospital/university can run anywhere from $35 to $80. This one is free, thankfully. Here is where you can find it.
From the methods section:
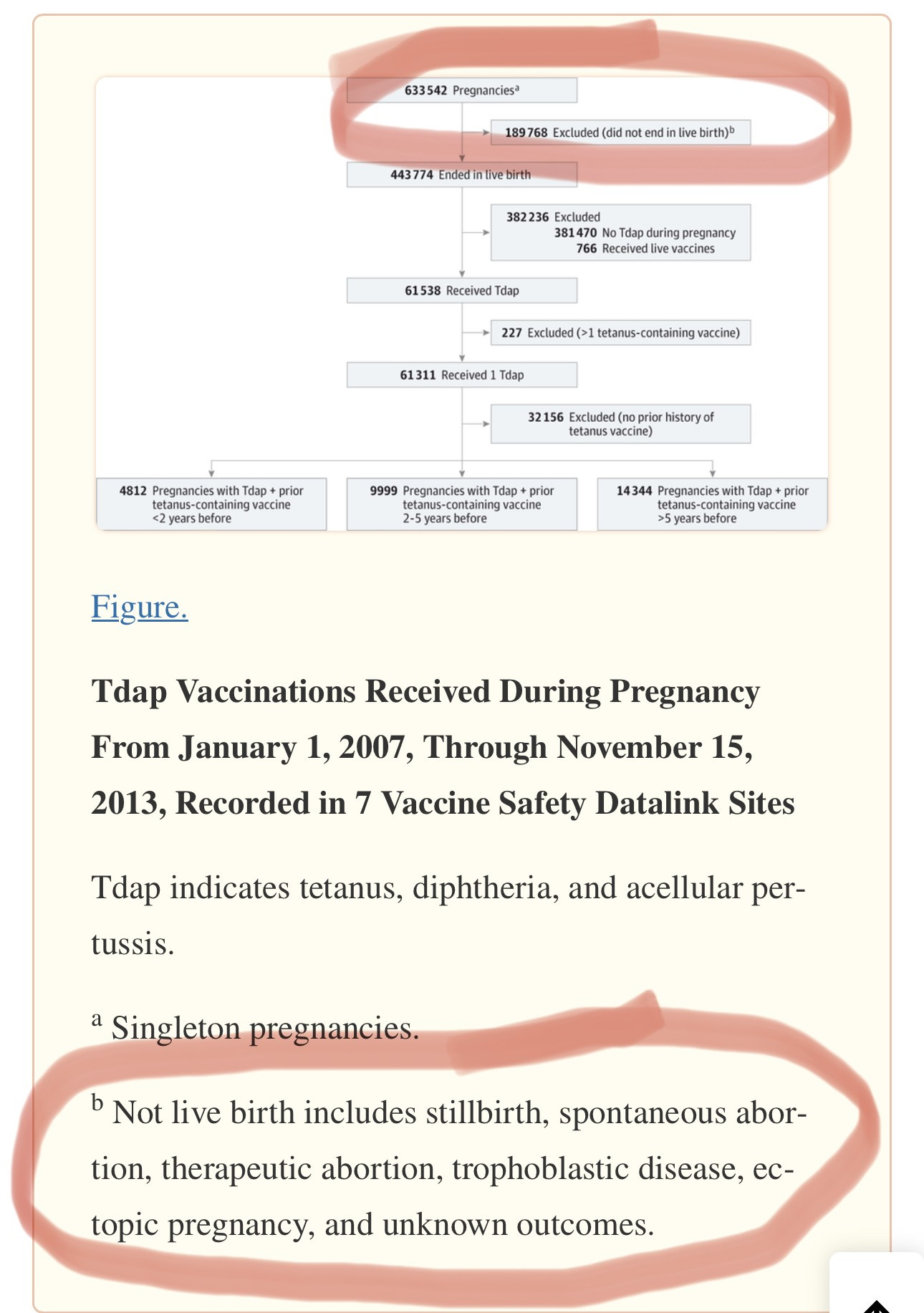
So, they started out with 633,542 pregnancies in their available pool of study subjects. They eliminated 189,768 pregnancies because they did not end in a live birth.
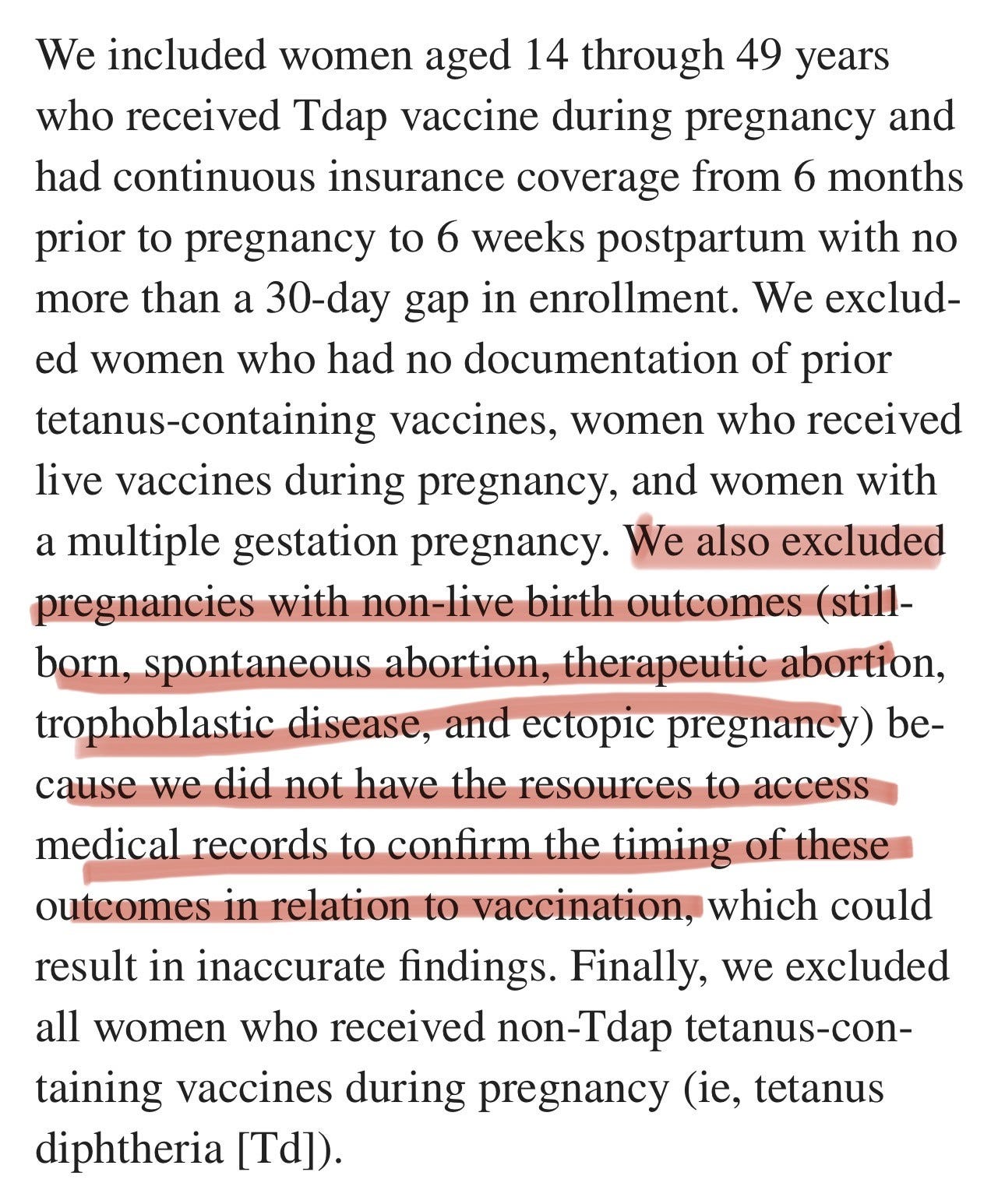
They eliminated nearly 200,000 pregnancies from their analysis because they did not end in a live birth. Among those pregnancies they eliminated were women who received a Tdap vaccine (and had received Tdap previously) and whose pregnancies ended in miscarriage (spontaneous abortion) and stillbirth. And their rationale for eliminating them was because “we didn’t have the resources to study that.” And then they have the GALL to report that repeated Tdap in pregnancy is “safe.”
One of the most important things to know, if you are considering receiving Tdap vaccination with every pregnancy, or even with ONE pregnancy, is whether or not doing so increases your risk of miscarriage or stillbirth. Yet, in this very large study, the researchers chose to exclude those women whose babies did not survive after their mothers were injected with Tdap vaccine. Why would they do that? Is it true that they “didn’t have the resources?” One bit of information we can look at to give us a clue about why they might have chosen not to study the most important safety outcomes is the Conflict-of-interest statement, which tells us who funded the research.
Here it is:
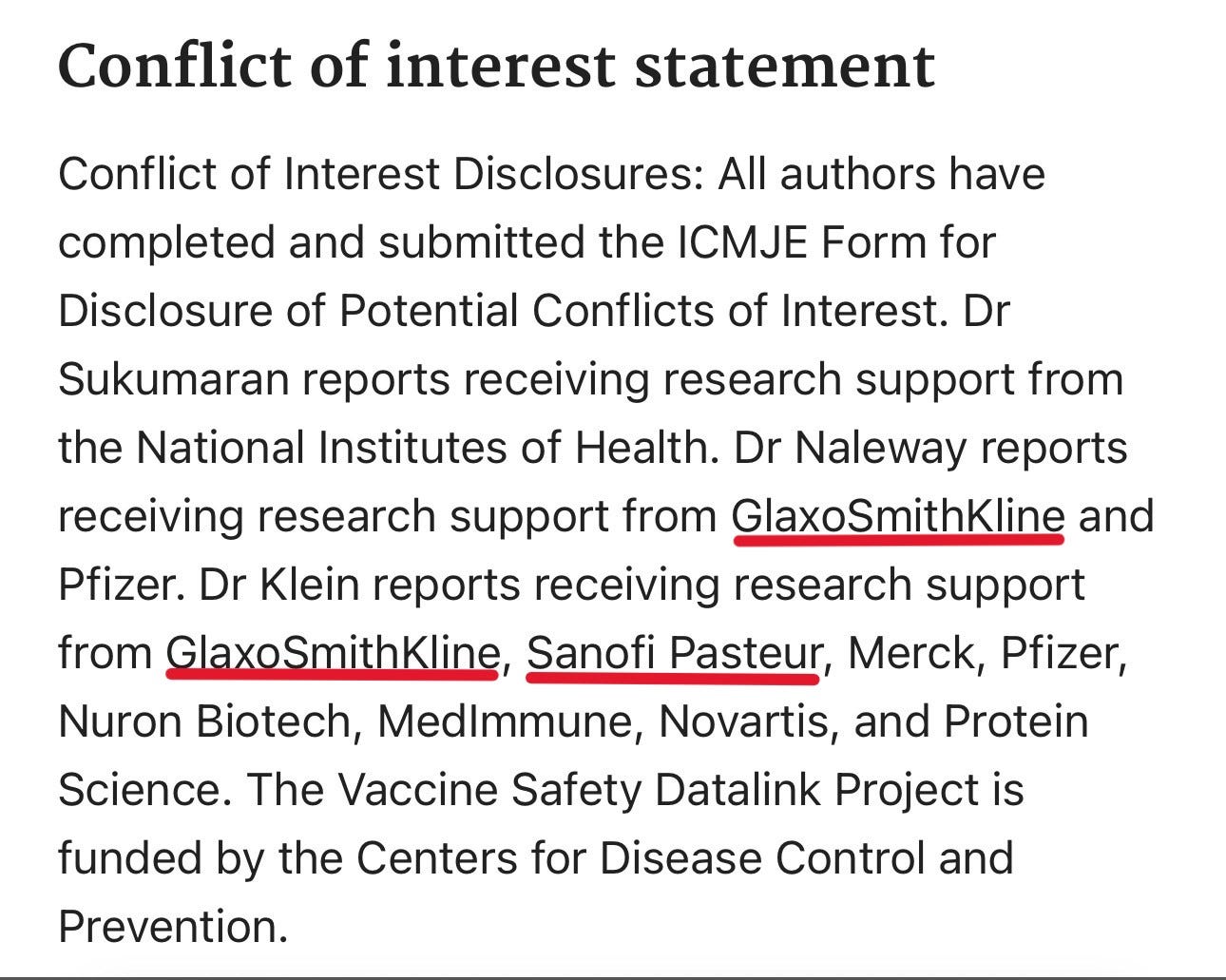
Who makes the Tdap vaccines that are given to pregnant women? In the United States, there are two options. Adacel is made by Sanofi Pasteur and Boostrix is made by GlaxoSmithKline.
The private sector cost of a single dose of Adacel is $47.83. Boostrix is $47.39. There are approximately 4 million babies born each year in the United States. This number does not include miscarriages or stillbirths. For ease of calculation, I will use the 4 million live births as the multiplier, and I will average the cost of Tdap at $47.50 per dose.
4,000,000 x $47.50 = $190,000,000
I would say that a hundred and ninety million dollars in sales per year is a very strong motivator that could have influenced the researchers to ensure their findings state that the Tdap vaccine in every pregnancy is “safe.”
Money is a very strong motivator for nefarious behavior in the research sector. But is it the only motivator? Is the money to be made from injecting pregnant women the only motivating factor for doing so? Are there other possible reasons for the increased push for Tdap vaccine, not only in pregnant women, but also in adolescents and young women? When we consider that the World Health Organization does NOT recommend boosters AT ALL after the initial childhood series (five shots between 2 months and age 4-6 years), and when we consider that the United States continues to push for Tdap in adolescence and every ten years after, if the motivation is not money alone, what is it?
Watch this video clip of Dr. Carrie Madej:
Here is where you can find the full interview.
Okay. That’s just nuts, right? Is there any documentation to support Dr. Madej’s claims? Yes.
As this article reports, in 2014, a mass vaccination campaign sponsored by WHO and UNICEF targeted 2.3 million Kenyan girls for vaccination against tetanus. The Catholic Doctors in the area got suspicious because the tetanus campaign was ONLY targeting girls and women, so they procured some of the shots and had them analyzed. They found HCG antigen, which is used in anti-fertility vaccines.
From the article:
According to a statement released Tuesday by the Kenya Catholic Doctors Association, the organization has found an antigen that causes miscarriages in a vaccine being administered to 2.3 million girls and women by the World Health Organization and UNICEF. Priests throughout Kenya reportedly are advising their congregations to refuse the vaccine.
“We sent six samples from around Kenya to laboratories in South Africa. They tested positive for the HCG antigen,” Dr. Muhame Ngare of the Mercy Medical Centre in Nairobi told LifeSiteNews. “They were all laced with HCG.”
Dr. Ngare, spokesman for the Kenya Catholic Doctors Association, stated in a bulletin released November 4, “This proved right our worst fears; that this WHO campaign is not about eradicating neonatal tetanus but a well-coordinated forceful population control mass sterilization exercise using a proven fertility regulating vaccine. This evidence was presented to the Ministry of Health before the third round of immunization but was ignored.”(source)
Recap: What we know about tetanus-containing vaccines…
All of the tetanus-containing vaccines contain aluminum and formaldehyde. Some also contain polysorbate 80 and mercury in the form of Thimerosal.
All tetanus-containing vaccines contain casamino acid from cow’s milk and present an elevated risk of anaphylaxis in children and adults who have allergies to cow’s milk.
The WHO does not recommend boosters of tetanus-containing vaccines after the initial five-shot series in childhood, and the published science indicates that there is ZERO difference in the incidence of tetanus in countries that give boosters vs. countries that don’t.
Changing the recommendations for boosters to every 30 years instead of every ten years would result in a savings of $1 Billion over four years.
The study that recommended changing to 30 years was published 8 years ago. If the United States had altered the recommended schedule based on the science, there would have already been a savings of $2 Billion.
The push for Tdap vaccine in every pregnancy is not based on adequate safety science, and there appear to be financial motives for not doing solid science, given that the manipulated studies are funded by the pharmaceutical companies that produce the vaccines.
Money does not appear to be the only motivating factor in the decision to continue promoting Tdap in pregnancy and in adolescence, with documentation that the Tdap vaccine has been used as a sterilization vaccine in other countries, without the knowledge or consent of the citizens who live in those countries. Is this the case in the United States, too??
Given that the research that is being used to demonstrate “safety” of the Tdap vaccine in pregnancy eliminated any pregnancies that ended in spontaneous abortion/miscarriage or stillbirth, if you are being pressured to get this vaccine while pregnant, I strongly urge you to read this article:
Fetal Demise: Deaths of Infants in the Womb Following Vaccination in Pregnancy

I have been putting off this post. Every time I think about writing about vaccines in pregnancy, I feel sick. My stomach churns. My breath becomes shallow. My heart rate quickens. And the tears come. And I start looking for something else to write about because it’s just too hard. But. It’s so necessary. And I have data that needs to be shared.
I hope this information is helpful to you as you attempt to navigate the lies and obfuscation that characterizes all aspects of the vaccine program. Please share this article.
For more information on the DTaP and Tdap vaccines, please read this article:
Let's Talk About Whooping Cough

This article was originally published on VaxTruth in 2015, following some big fear-mongering in the mainstream news over outbreaks that took place in 2010-2015 and which were being blamed on “unvaccinated children.” What follows is an updated version of that article.
My child hasn’t had any vax since 2017 and now is required to get a tdap booster to advance to the next grade….we’re doing homeschool instead. Thank you for giving me more information to solidify our decision.
My 81 year old MIL was given a *tetanus shot when she fell in her own bathroom and broke her pelvis. This was during the COVID crap and they were limiting the number of people in rooms. What a pathetic system it has become. 💰